45 years ago today, Mount St. Helens erupted. From my home in Tacoma over 70 miles away, I could hear and feel the blast and see the plume of ash, rock, and hot gases rising into the atmosphere.
Such major blasts of chaotic energy and hot gases produce extensive damage. The explosion darked the skies for miles, extinguished lives, erased forests, and rearranged the landscape. The melted glacial ice generated a lahar that carried away homes, destroyed highway bridges, and clogged shipping lanes. The blast left behind tons upon tons of pulverized rock that continue to cause challenges for communities living downstream–such as clogging their drinking water systems.
Mount St. Helens is now one of the most closely monitored volcanos in the world. Last Saturday at the Cascade Volcano Observatory (CVO) open house I learned about different types of volcanoes, effects of eruptions on living creatures and the earth, how we track and model earthquakes to predict eruptions, understanding lahar flows so we can provide early warnings, and atmospheric influences on that guide ash and volcanic gas distribution. Models for making these predictions depend on data gathered by a variety of sources, such as weather balloons launched by the National Oceanic and Atmospheric Administration (NOAA). We can’t prevent volcanoes from erupting, but we can improve our preparedness and detection abilities so we can help reduce deaths and damage–IF we can learn from history and maintain the will to and funding to do what is necessary.
The posters I’m sharing in this blog were on display at the CVO open house. CVO is part of the Volcano Hazards Program run the by U.S. Geological Survey (USGS), which is under the U.S. Department of the Interior. Many USGS scientists and staff have departed in response to government actions of the past few months. In May the federal government has notified USGS researchers and students that their funds could be frozen and staff could be laid off. Other government cutbacks (such as reduced weather balloon launches) reduce USGS ability to monitor volcano activity, not to mention the U.S. Weather Service’s ability to predict tornadoes and other severe weather.
Despite the devastation, signs of life returned to the desolate blast zone within months, but it will never appear as it did before the eruption. If we don’t actively pursue the objective study of our world, we not only limit our learning about the world we live in, we will become less able to predict impending disasters and protect lives. Guess we’ll just have to adapt when natural disasters strike. If we can.
In early June, the American Society of Clinical Oncology held its 2022 Annual Meeting (#ASCO22) in Chicago. This was the first in-person annual meeting since the pandemic began. While attendance was smaller than usual, McCormick Place (the largest convention center in North America) still hosted 30,000 oncology-related clinicians, researchers, healthcare professionals, patients, and advocates from all over the world.
To address the risk of COVID-19 transmission, attendees were required to prove they were fully vaccinated against COVID-19. Attendees also were required to have a negative COVID-19 test, and COVID tests were readily available during the conference. Masking was recommended – “ASCO expects all attendees to be masked indoors at our meeting when not eating, drinking, or presenting.”
I am a cancer research advocate living with incurable lung cancer for over eleven years. I started attending ASCO Annual Meetings in 2014. It’s wonderful to gather with other cancer patient advocates, network with oncology professionals, and learn about the newest research for my disease. I would have loved to attend in person this year, but I didn’t. I chose to attend virtually during the pandemic because my radiation-scarred lungs are prone to infection (I’ve had pneumonia more than once since my diagnosis), and lung cancer patients are at increased risk of death from COVID-19. However, I had a window into the happenings at McCormick Place via the #ASCO22 hashtag on Twitter, as well as texts and messaging from friends who were there.
Many attendees tweeted pictures of colleagues reunited after a long, trying absence. The pandemic has been especially tough on medical professionals. They needed the joy that reconnection brings. I don’t begrudge them that.
However, those images generated a different emotion for me. After speaking with several friends in the lung cancer patient advocate community, I’ve learned I’m not alone in my feelings.
I’m pissed that the ASCO community appears to have given so little value to the safety of people who have cancer. Here’s why.
RISK OF COVID-19 TRANSMISSION AT #ASCO22 WAS KNOWN BEFOREHAND TO BE HIGH
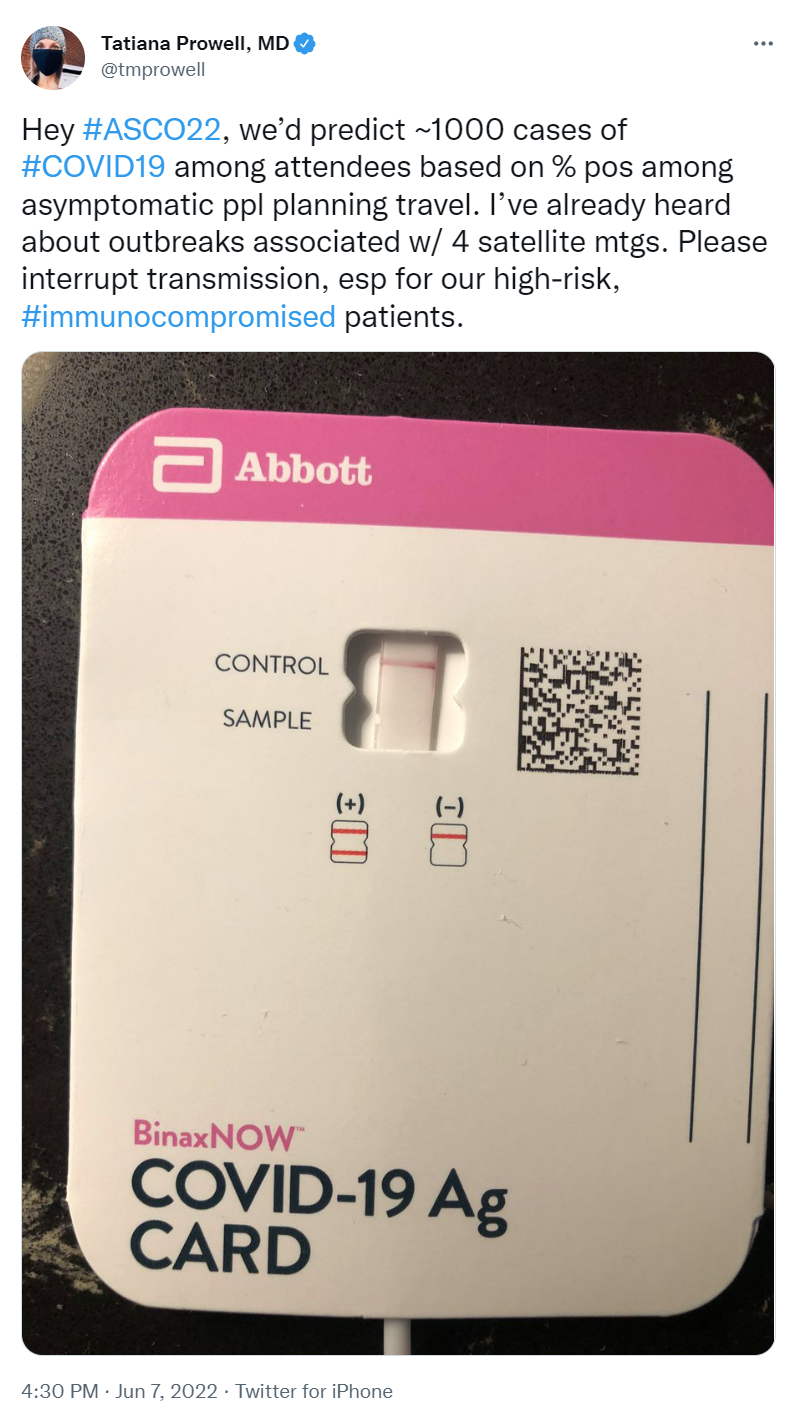
COVID-19 transmission was deemed high in Chicago by the city’s COVID Dashboard in the weeks leading up to #ASCO22. Omicron variants were on the rise and deemed very transmissible. With tens of thousands in attendance, chances of encountering someone infected with COVID were NOT low. Although omicron symptoms seem generally less severe, people are still dying from it–especially people with underlying conditions, like cancer. Others have lingering side effects.
Several medical professionals who attended the smaller 2022 American Association of Cancer Research (#AACR22) Annual Meeting in New Orleans last April tested positive for COVID-19 a few days after the meeting. Masks were not required at AACR, and few masks were seen in surrounding hotels, restaurants, and public transportation. By the start date of the much larger ASCO meeting two months later, community transmission of COVID was much higher. The likelihood someone at #ASCO22 would become infected was a virtual given.
MASKS WERE EXPECTED, BUT NOT REQUIRED
While ASCO expected masks to be worn, masking was not required nor enforced. On the second day of the conference, a tweet observed that perhaps 50% of attendees were wearing masks. Other tweets showed some attendees gathered for selfies and group pictures in session rooms and hallways wearing no masks. Others reported people at ancillary events and hosted parties that included food were frequently unmasked.
ONLY ONE COVID-19 TEST WAS REQUIRED, AND RESULTS WERE NOT CHECKED
ASCO 2022 required a COVID-19 test “within 48 hours of the time they entered any of the session rooms or exhibit hall.” This allowed international attendees with long flights to test after they arrived at McCormick Place. However, testing relied on the honor system: no one verified nor recorded test results. Both rapid and PCR tests were readily available throughout the conference for those who wished to test again, but no system was available for posting results. One doctor who planned to attend tested negative for COVID the day before travel. To be extra safe, they tested just before leaving for the airport. That second test was positive. As a result, she chose not to attend the conference.
It’s unlikely everyone was equally diligent with testing. How many people arrived at the conference unknowingly positive?
ONCOLOGY PROFESSIONALS, YOUR PATIENTS WANT YOU TO SET THE EXAMPLE
Oncology is a medical field that’s evidence based and highly dependent on data. Good results demonstrated in clinical trial data are essential to getting new cancer drugs approved by regulators and available to patients. One would think oncology professionals would be the first to follow the data when it comes to protecting their patients from COVID-19. People who have cancer expect our doctors, nurses, and other clinical professionals to set and maintain a high bar.
So many patient advocates typically attend ASCO that the meeting offers a Patient Advocate Lounge as well as patient-focused programs. Many of these advocates have active cancer. Before the meeting, both patient advocates and doctors pleaded with ASCO to make masking a requirement to reduce the risk of spreading of COVID to patients who attended ASCO, and to healthcare providers at ASCO who would be seeing patients in clinic when they returned home. ASCO refused. The letter has since been taken down, but is mentioned in this article.
Lung cancer patient and research advocate Jill Feldman had the honor of being invited to speak in an ASCO education session. Including patients on ASCO panels is still rare, and Jill takes the responsibility of representing the patient voice seriously. She chose to forego in-person ASCO except for the session in which she was speaking because she had significant COVID anxiety — she’d been hospitalized for the virus last December. She lives near Chicago, so she didn’t have to fly or stay in a hotel. She wore an N95 mask, except for her time on the podium. A tweeted picture of the audience in her session (since deleted) showed many faces and few masks. Despite Jill sharing her anxiety about possible COVID exposure at the end of her talk, some ASCO attendees approached her afterwards to chat without wearing masks.
I am grateful for the oncology professionals who are caring for me. I am glad they feel renewed by their experience at #ASCO22. I appreciate those who were careful to stay masked while at the conference.
Still, I am angry about the apparent disregard for people who have cancer that was demonstrated by ASCO as a community and the oncology profession as a whole. Many #ASCO22 attendees were unmasked while hugging, sitting shoulder-to-shoulder in sessions, chatting while in noisy food courts, catching up over Exhibit Hall lattes, and networking at after-hours parties. I wonder how many of them (or the people they were near) were in clinic the next day sharing their ASCO joy and COVID with immunocompromised patients.
A fellow lung cancer advocate and virtual #ASCO22 attendee tweeted her decision not to attend in person. Her choice was widely applauded: in five days, her tweet received almost 2000 likes, 200+ retweets, and dozens of “thank you” responses.
C’mon, ASCO community, you can do better. Cancer patients expect – no, REQUIRE – you to set a high bar. Step up.
The first case of COVID-19 in the USA was reported on 1/20/2020—over 9 months ago. Since then, the country has reported 9,860,558 cases and 237,113 deaths (per Johns Hopkins). As the weather becomes cooler and we spend more time indoors, the number of cases is rapidly accelerating in almost every state.
Given this surge, holiday gatherings and activities present a serious risk for virus transmission. On November 5, 2020, the #LCSM (Lung Cancer Social Media) Chat community on Twitter discussed ways to enjoy and celebrate the holidays safely during the pandemic. Chat participants included lung cancer patients, caregivers, advocates, physicians, and healthcare workers. The chat, which included links to many helpful resources, covered the following topics:
What have we learned over the past 8 months about how COVID-19 is transmitted?
How can people reduce the risk of COVID-19 during outdoor activities?
How can people reduce the risk of COVID-19 when travel is involved? What about travel to or from hot spots?
How safe is it to meet with family and friends who had COVID-19 and recovered?
How can people reduce the risk of COVID-19 for indoor activities (shopping, dining in restaurants, family gatherings, worship services, etc.)?
When people flee urban areas to second homes or rural areas to avoid the COVID-19 pandemic, they put the locals who live permanently in the area of their “disaster” home at risk, and strain local services. Small town groceries are not designed to supply large populations. Small town medical center are not equipped to handle several (if any) critically ill people. Rural Internet does not have the capacity to support work from home or streaming video.
“Shelter in Place” and “Stay at Home” do not translate as “travel to an escape home.” You’re supposed to stay put and avoid spreading the disease.
It doesn’t matter that you feel healthy. Current estimates say 50% of people who are infected with the novel coronavirus will exhibit absolutely no symptoms, yet they are still able to spread COVID-19 to others. And some who feel healthy today might develop symptoms in the next two weeks.
The content below was posted by several lung cancer advocacy groups today. Shared with permission.
We understand and appreciate the severity of the new coronavirus epidemic (also known as COVID-19) that’s spreading globally. As advocacy organizations dedicated to serving the needs of lung cancer patients, all of us are closely monitoring the latest developments related to the outbreak caused by the novel coronavirus, SARS-CoV-2, and the resulting disease, COVID-19.
This is a rapidly evolving situation and we are following updates provided by the World Health Organization (WHO) and the US Centers for Disease Control and Prevention (CDC), which can be found here:
This novel virus presents a unique threat to vulnerable populations, including the elderly and those with weakened immune systems, including cancer patients. Early studies conducted on lung cancer patients undergoing surgery suggest that this virus readily infects the lungs and can potentially cause pneumonia, making lung cancer patients particularly susceptible. 1
Research suggests that the overall clinical consequences of COVID-19 may ultimately be similar to those of a severe seasonal influenza or a pandemic influenza.2
What you can do:
First and foremost, we encourage everyone to follow best practices for public health, such as staying home when ill, handwashing with soap and water (or using a hand sanitizer), and respiratory etiquette including covering the mouth and nose during sneezing and coughing.3 Many of the steps you would take to protect yourself from catching the flu also apply for protecting yourself against COVID-19.
Regarding travel within the United States, at this time there are no restrictions on travel. However, the situation may change rapidly. We encourage all people to evaluate the need for non-essential travel and to take appropriate precautions if travel is required. Please check with your doctor before making international travel plans. Again, the CDC is maintaining a page that outlines current travel advisories: https://www.cdc.gov/coronavirus/2019-ncov/travelers/index.html
What you should not do:
Do not read or share information about COVID-19 from websites that are not maintained by reputed public health organizations (for example, the CDC). When in doubt, check your facts with what’s posted on the CDC or WHO website.
Resources and websites:
You can find information specific to your state or city or town on your health department’s website.
Tian S, Hu W, Niu L, Liu H, Xu H, S. X. Pulmonary pathology of early phase 2019 novel coronavirus (COVID-19) pneumonia in two patients with lung cancer. Journal of Thoracic Oncology. 2020.
Fauci AS, Lane HC, Redfield RR. Covid-19 – Navigating the Uncharted. N Engl J Med. 2020.
Del Rio C, Malani PN. 2019 Novel Coronavirus-Important Information for Clinicians. JAMA. 2020.
GO2 Foundation for Lung Cancer (amoore@go2foundation.org)
LUNGevity Foundation (ubasuroy@lungevity.org)
Lung Cancer Foundation of America (KNorris@lcfamerica.org)
Lung Cancer Research Foundation (jbaranski@lcrf.org)
LungCAN (kimberly@lungcan.org)
This Photo by Unknown Author is licensed under CC BY-SA-NC
Fellow travelers (especially those with cancer or other health issues):
Given the worldwide spread of measles, please be sure you have immunity to measles. You might need an MMR (Measles Mumps Rubella) booster vaccine.
The global measles outbreaks have demonstrated the measles virus can be spread by travelers. You, as a traveler, can be exposed to the disease. However, if you do not have immunity, you can also expose others to the disease. A single traveler carrying the measles virus can expose a local population even before the traveler has symptoms of the disease. It doesn’t have to be international travel — any travel to another location risks spreading the disease to a new population.
The CDC claims “If you and your travel companions have received two doses of a measles-containing vaccine (and can document both of them), you have sufficient protection against the disease. You do not need any additional measles vaccines or lab work. You are also protected against measles if you have laboratory evidence of immunity, laboratory confirmation of measles disease, or if you were born before 1957.”
In the case of Baby Boomers or those dealing with chronic or serious health conditions, I would go further.
I was born before 1956, so the assumption would be that I’m immune to measles. However, since I have compromised lungs due to lung cancer treatment and Washington State had a measles outbreak last year, I asked my PCP about my immunity. She recommeded I have a titer to test whether I still have immunity to measles, mumps and rubella. The tests only required a blood draw, followed by a separate analysis of immunity for each disease.
My titers showed I still had immunity to measles and rubella, diseases which I had as a kid. However, I’ve never had mumps. Even though I had the MMR vaccine when I was 17, the titer showed I had lost my immunity to mumps. Because of my level of immunity and my previous MMR, my doctor prescribed a single MMR booster shot. The cost of all three titers and the MMR booster were completely covered by my insurance (a BCBS company).
My son is in his 30’s, and had the MMR vaccine as an infant. He never had any of these diseases, although he did get chicken pox. His titers showed he was immune to two diseases, but had lost immunity to the third. His doctor recommended a single MMR booster. His insurance (Kaiser) covered the titers and MMR booster for him as well.
Please, if you plan to travel, make sure you have immunity to measles. More information is available here:
Have you or a family member been diagnosed with lung cancer?
Are you already active in providing lung cancer support and/or education to others?
Do you want to ramp up your advocacy work and learn more about the science of lung cancer research?
THEN …
Apply for the brand-new STARS (Supportive Training for Advocate in Research and Science) program! STARS was developed by the IASLC (International Association for the Study of Lung Cancer) in collaboration with international lung cancer patient research advocates and advocacy nonprofits.
Those accepted in the program will be assigned a mentor from their own country, meet and learn lung cancer science from researchers, develop science communication skills, and attend the World Conference on Lung Cancer (WCLC) in Barcelona, Spain in September 2019.
Life as a lung cancer research advocate can require a lot of travel. This week I’m in Washington DC for two meetings.
Monday I participated as the sole patient advocate in the National Cancer Institute’s Small Cell Lung Cancer (SCLC) working group meeting, along with some of the top US researchers in this disease. The meeting will provide fodder for the NCI’s report to Congress about the Recalcitrant Cancers Act.
Thursday I’ll be one of several patient advocates at the National Institutes of Medicine for a meeting on data sharing, along with medical institutions, pharma, and healthcare payers. Data sharing in the electronic age involves more than just who can see your medical records. We patients and family members have already participated in several phone calls in preparation for this meeting. It will be interesting to hear what the other stakeholder groups think are the main barriers to data sharing, and what we should do about them.
In between, I’m trying to get caught up on expense reports and writing projects while adjusting to a new time zone. I hope my inputs make a enough difference for patients to make the travel worthwhile.
If you’re a cancer patient looking for assistance with paying for targeted therapies, transportation to appointments, lodging near cancer centers, or other issues, check out Nancy’s List of financial assistance resources!
Chemist Jean Cui at #ASCO17 posters with #ALK & #ROS1 NSCLC patients who thrive on drugs she helped develop
As cancer patients and caregivers transform into active cancer advocates, they may think about attending medical conferences. On March 8, at 8 pm Eastern Time (5 pm PST), #LCSM Chat will discuss various aspects of cancer advocate participation in medical conferences.
Some reasons for cancer advocates to attend medical conferences are to:
Learn more about cancer and treatment options for cancer
Get details about new research
Meet the top doctors who treat their type of cancer
Support an advocacy organization’s outreach booth
Network with other advocates, as well as clinicians and researchers
Share an advocate’s perspective on a specific topic, sometimes as an invited speaker
As more advocates participate in conferences, the conference organizers, professional societies, and medical practitioners are coming to understand the benefits of including advocate voices in their programs. #LCSM Chat member Janet Freeman-Daily was recently interviewed by the International Association for the Study of Lung Cancer about her participation in conferences–read the resulting article here: Why Should Advocates Attend Academic Lung Cancer Conferences?
Tools exist to help advocates navigate cancer conferences and understand the content they will see:
If you know of other resources, please share them in the comments on this page or in the chat.
Some professional societies and cancer nonprofits sponsor programs that enable cancer advocates to attend conferences and learn more about medical research:
AACR’s Scientist↔Survivor Program
Participants receive travel grants and participate in special educational programs at cancer research meetings.
ASCO’s Conquer Cancer Foundation Patient Advocate Scholarship Program
Provides need-based grants to cover travel and registration for a variety of ASCO meetings, including the huge Annual Meeting in Chicago each June. Applications for the Annual Meeting are usually accepted during a window in early March.
RAN’s Focus on Research Scholar Program
Scholars participate in preparatory conference calls, virtual classroom (webinars), learning materials and mentoring for research advocates to improve skills and understanding of biomedical research, and attend the ASCO Annual Meeting.
International Association for the Study of Lung Cancer (IASLC) Travel Awards for World Conference on Lung Cancer (WCLC)
Provides travel grants to WCLC, which is held in a different international city each year—it will be in Toronto Canada September 2018.
Our moderator Janet Freeman-Daily (@JFreemanDaily) will lead our discussion using the following prompts:
T1: When a cancer patient/caregiver attends a medical conference, what are benefits to the patient/caregiver? Benefits to medical professionals? To the conference?
T2: If you have attended a medical conference in which patients/caregivers participated, what did you like most about that conference? (Pls state whether you attended as patient, caregiver, or med professional)
T3: If a cancer patient or caregiver wanted to attend a medical conference, which would you recommend for their first conference, and why?
T4: What tips would you give a cancer patient or caregiver for making the most of their conference experience?
T5: What programs help cancer patients and caregivers attend and/or afford conferences? Do you have experience with any of them?
We hope you’ll join our #LCSM Chat on Thursday 3/8 at 8 pm Eastern Time (5 pm Pacific). If you’re new to tweet chats, please read our primer “To Participate in #LCSM Chat.”































{kind=link}