This year’s Targeted Therapies in Lung Cancer Patient Forum is happening online Saturday June 15, and it’s FREE! Great way to learn about current treatment options for those eligible for targeted therapy.
This signature, live, virtual, interactive patient education event includes presentations and panel discussions covering general subjects relevant to all targets as well as breakout sessions on specific mutations of lung cancer. Save your spot here: [https://give.cancergrace.org/…/targeted…/e490332](https://t.co/8TDXsdjyp5)
Lung cancer research gives patients hope, time with loved ones, and better quality of life. Ten years ago today, I entered a targeted therapy clinical trial for my ROS1+ lung cancer, taking an oral drug called crizotinib (trade name Xalkori). I’m still taking it (it’s now approved by the FDA and in many other countries) and have had no evidence of disease since I started it. Pretty amazing, since I had been given an expiration date of 2 years at the outside for my metastatic non-small cell lung cancer.
Many of my friends who have lung cancer take targeted therapy pills. Mine costs $17K per month when not covered by insurance. Some drugs cost even more.
Unfortunately, most all patients who take targeted therapy pills see their cancer eventually start to grow again. These patients often must change to a different anti-cancer therapy. When a patient has to change therapies, they may be left with unused medications.
Patients on expensive medications HATE to throw out their cancer drugs when those same drugs might help someone else live longer or more comfortably.
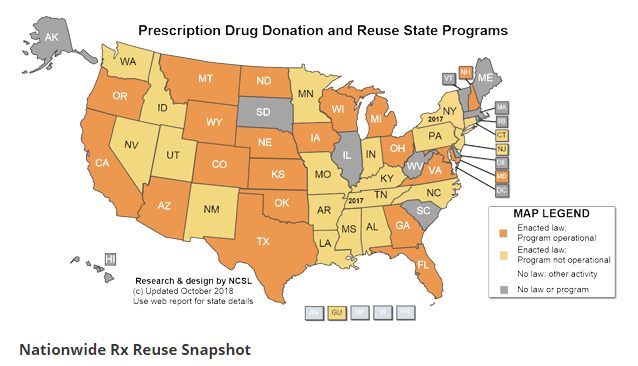
Some US states will allow “prescription reuse” — unopened cancer drugs can be donated for use by a different patient. As the map shows, state laws on this subject vary significantly, and not all states that have enacted prescription reuse laws have operational programs that enable reuse.
Why isn’t this easier? Why can’t I just drop off my unused pills at a pharmacy and know they’ll get to someone who really needs them but can’t afford them?
If you wish to donate unneeded cancer drugs, check with a local pharmacy or prescriber for practical advice on what may work in your situation, in your state. If your state has no operating program, contact your state legislators.
What a great opportunity for patient advocacy to make a difference!
The original ROS1ders: Stuart Grief, Lisa Goldman, Tori Tomalia, Janet Freeman-Daily, Lysa Buonanno
I first “met” my friend Tori Tomalia in an online lung cancer community in 2013. A gifted writer, she already had a well-established blog that was funny, informative, and poignant. I admired the way she sculpted words to show how life continued despite all the downsides that accompany a deadly disease.
Tori was diagnosed with ROS1+ lung cancer about a year after me. We formed a connection through blogging and shared lung cancer advocacy activities, such as promoting #LCSM (Lung Cancer Social Media) Chat on Twitter. Her blog explored areas of life that I would never know: how to tell your young child you have a deadly cancer, how to make memories with the kids when you feel like crap. Her lung cancer journey was much different than mine. She had recurring brain mets that required radiation and sometimes brain surgery. While my clinical trial drug gave me years of no evidence of disease, for her it caused constant nausea. Clinical trial drugs failed her quickly. Yet her blogs and social media posts, though honest and at times raw, often found something positive to share, even if it was that she was still alive. Tori embraced life.
The first time Tori and I met in person was when five ROS1+ cancer patients found each other in a bar at LUNGevity Hope Summit in April 2015—a gathering that sparked the creation of The ROS1ders. I don’t remember much of that whirlwind weekend in Washington DC, but I clearly remember chatting with her on the bus coming back from the awesome Saturday dinner at a historic carriage house. Her quiet confidence inspired me. As I got to know her, I learned about her fierce inner advocate, ability to get the job done, and devotion to family. I also learned we shared a love of Buffy the Vampire Slayer.
Shortly after that event, Tori set up the private Facebook group that became the focus of The ROS1ders. She was often the first person with whom new members interacted; she had a gift for making them feel welcomed and hopeful through a computer screen. As we worked together, Tori often brought sparks of insight and inspiration to our discussions. She coined our name “The ROS1ders,” revised posts to make them understandable to a greater number of people, and frequently provided a reasoned, compassionate alternate viewpoint. One time when we needed a post to describe using mice to study our cancer, I asked Tori if she would write it. She was nervous about it, pointing out that she and I had different writing styles (I tended towards science geek, while she tended towards improv comedy). I told her different styles kept things interesting, and I knew I’d like whatever she wrote. When the blog was posted, I actually laughed with delight at her chosen title: “The ROS1ders meet the rodents.” (You were wondering why the title referenced rodents? Now you know.)
I think The ROS1ders have succeeded as much as they have because of the indescribable bond that the cofounders Tori, Lisa Goldman, and I shared. We never had a fight. We just talked things through. I feel blessed to have experienced this magic.
I was thrilled in 2018 when Tori and I discovered our clinical trial visits to the University of Colorado in Denver would be happening at the same time! I eagerly waited in the DIA terminal for her flight to arrive. As she came off the elevator, she gave me a big smile, and I smiled in return at her awesome high-top red-sequined sneakers (reimagining Dorothy in the Wizard of Oz). I played chauffeur for her that trip, and helped her navigate the CU campus as she went through all the tests and procedures required to enroll in the trial. We connected on a few more trips after that, including one where she accompanied me to the offices of the International Association for the Study of Lung Cancer and helped with early planning for the STARS program (which she named). Eventually Tori was able to move her clinical trial participation closer to home in Michigan. We didn’t see each other in Denver again.
My last meeting with Tori was in New York City in May 2019, when The ROS1ders were finalists for a precision medicine award. Tori and I wandered around NYC near our hotel looking for a mutually agreeable take-out restaurant. Later, we connected with Lisa Goldman and another ROS1der, Jess Wittebort, in the park outside the NY Public Library (where the event was held). We talked about life, death, and everything in between. We could talk about anything. It was a wonderful evening.
Tori did everything she could to stay in this world and share the adventure of living with her beloved husband, children, and extended family. In the end, the weariness of years dealing with treatments and side effects wears one down. I hope this story helps her children see the side of Tori that was so dedicated to helping others live better and longer despite ROS1+ cancer.
Zander, Mikaela, and Autumn: Your mama is amazing. She made a difference to hundreds of people. Thanks for sharing her with the lung cancer community.
I’m excited to participate in the STAT News video chat “What gene targeted therapies mean for patients with cancer” on April 8, 2021 at 1:00 p.m. ET (10:00 a.m. PT) on the topic The discussion will include a great group of speakers:
Bonnie J. Addario, lung cancer survivor; co-founder and board chair, GO2 Foundation for Lung Cancer
Narjust Duma, M.D., assistant professor of medicine, thoracic oncology, University of Wisconsin Carbone Cancer Center
Janet Freeman-Daily, MS, Eng, co-founder and board chair, The ROS1ders; stage IV lung cancer survivor & research advocate
Laura A. Petrillo, M.D., palliative care physician, Massachusetts General Hospital and Harvard Medical School
Camille Hertzka, VP, head of oncology U.S. medical, AstraZeneca (sponsor speaker)
Eric Boodman, general assignment reporter, STAT (moderator)
The US FDA is hosting a listening session to gather patient perspectives on oncogene-driven lung cancer. Representatives from several biomarker patient groups will speak; I will be speaking on behalf of The ROS1ders. Representatives from the FDA will share ways they are addressing the concerns raised by the patients.
The virtual 2020 IASLC North American Conference on Lung Cancer (NACLC 2020) runs October 16-17. Patients will be providing special perspectives throughout the conference.
The eight-hour virtual cancer research conference started at 5:45 AM
AND
The livefeed repeatedly crashed
AND
A researcher mansplained how to handle the survey that you just helped design
AND
A conference presenter says the targeted therapy cancer drug that is keeping you alive is too costly, and chemo (which didn’t work for you) is just as effective
AND
Someone in your international lung cancer patient support group dies for lack of access to drug that is standard of care in your country
AND
A local friend gets diagnosed with metastatic lung cancer
AND
A friend of another friend gets diagnosed with stage 4 breast cancer.
Ever wonder what happens at the annual IASLC Targeted Therapies in Lung Cancer (#TTLC20) meeting in Santa Monica, California? To mark the meeting’s 20th Anniversay this week, I chatted with two of the co-chairs, Drs. Paul Bunn and Suresh Ramalingam, on the IASLC “Lung Cancer Considered” podcast. Listen or download here:
The overall cancer death rate has been falling about 1.5% a year since 1991. It fell 2.2% from 2016 to 2017, according to the new American Cancer Society report. That’s the largest drop ever seen in national cancer statistics going back to 1930, said Rebecca Siegel, the lead author. ‘It’s absolutely driven by lung cancer,’ which accounts for about a quarter of all cancer deaths, she said. Take lung cancer out of the mix, and the 2017 rate drop is 1.4%, she added.
Experts mainly credit advances in treatment. Topping the list are refinements in surgery, better diagnostic scanning, and more precise use of radiation.
They also celebrate the impact of newer drugs. Genetic testing can now identify specific cancer cell mutations, which allow more targeted therapy using newer pharmaceuticals that are a step beyond traditional chemotherapy.
This news reinforces National Cancer Institute (NCI) data published in 2019 that the lung cancer 5-year survival rate rose to 19.4% for all types of lung cancer. When I was diagnosed with lung cancer in 2011, the 5-year survival rate for lung cancer was only 16%, and the majority of lung cancer patients survived less than one year. As the STAT article says, it has a LOT do with newer lung cancer diagnosis and treatment options. A major contributor is genomic testing of tumors, and the targeted therapies that can inhibit cancer cells driven by altered genes. Patients on some targeted therapies have a median survival of over five years! About 30% of non-small cell lung cancer patients are currently eligible to take some form of targeted therapy, and that number may soon rise to 50%.
The benefits of targeted therapies have just begun to affect the NCI’s five-year survival stats. The first successful lung cancer targeted therapy clinical trial (crizotinib for ALK-positive non-small cell lung cancer) began in 2007, and the drug was approved in 2011. The NCI’s 2019 stats are based on data collected between 2009 and 2015. The survival rate will continue to go up due to approval of more targeted therapies, as well as the advent of immunotherapy (first approved in 2014), more precise radiation treatments, better surgical techniques, and early detection with lung cancer screening. When lung cancer is caught in early stages, 80% of patients are CURABLE.
However, despite obtaining their information from same source (the Associated Press), some media outlets have emphasized different angles of this story. An National Public Radio (NPR) article states, “What’s behind the decline [in cancer deaths]? In part, smoking rates have fallen steadily, which means the biggest risk factor for lung cancer has fallen appreciably. New cancer treatments are also playing a role, Siegel says.” (That’s ALL NPR’s article says about the contribution of better lung cancer treatment to the reduction of cancer deaths).
I wish the media would stop emphasizing smoking cessation as the cure for lung cancer death, instead of the significant advancements lung cancer treatment. Anyone with lungs can get lung cancer. An increasing number of lung cancer cases (currently around 20%) occur in never smokers. While overall lung cancer deaths have been dropping slightly, the death rate in young women who have never smoked is actually RISING. The World Health Organization has acknolwedged that air pollution is a risk factor for lung cancer, as is exposure to radon gas and other environmental exposures.
Crediting smoking cessation as the primary reason for reduction in lung cancer deaths perpetuates stigma, which contributes to worse lung cancer outcomes through physician nihilism, patient anxiety depression, and reduced funding for lung cancer research. Once a person has been diagnosed with a serious disease, they should receive the same compassion and treatment regardless of their personal characteristics. Blaming the patient and telling them to stop smoking never cured anyone. But it may prevent the patient from experiencing the best possible outcome for their disease. Why won’t the media emphasize very real contribution–and the hope–offered by better lung cancer treatments ?
So, when you see news about the reduction in cancer deaths (and lung cancer in particular), please look past the errant “due primarily to smoking reduction” emphasis. Focus instead on the hope offered by cancer research and the increasing number of new lung cancer therapies. We don’t have a lung cancer cure for everyone, but researchers are working on it. Those touched by lung cancer need that hope.
We’re getting better at killing lung cancer. Stigma is SO much harder to kill.