Lung cancer research gives patients hope, time with loved ones, and better quality of life. Ten years ago today, I entered a targeted therapy clinical trial for my ROS1+ lung cancer, taking an oral drug called crizotinib (trade name Xalkori). I’m still taking it (it’s now approved by the FDA and in many other countries) and have had no evidence of disease since I started it. Pretty amazing, since I had been given an expiration date of 2 years at the outside for my metastatic non-small cell lung cancer.
Proud to have co-authored this print article about expert patient contributions as educators, advocates, and research partners! Thanks to Collaboration for Outcomes using Social Media in Oncology (COSMO) for the opportunity.
The IASLC STARS program invites STARS alumni and anyone interested in cancer research advocacy to join us for a webinar about cancer drug development.
When: Monday August 29, 2022, at 11:00AM Eastern Time
Title: Advocacy Opportunities in Cancer Drug Development and Regulatory Approval
Speakers: Upal Basu Roy, PhD, MPH, Executive Director of Research, LUNGevity Foundation Janet Freeman-Daily, MS, Eng cancer research advocate and STARS staff (moderator)
Languages: English, with transcript translated into Spanish after the event
Learning objectives:
Acquire a high-level understanding of the drug development process and timeline
Identify differences in global regulatory approval pathways and how they impact drug access
Identify advocacy opportunities throughout the drug development process
The International Association for the Study of Lung Cancer (IASLC) offers webinars, training and networking opportunities to lung cancer research advocates through its Supportive Training for Advocates in Research and Science (STARS) program. Thank you to our STARS partner Research Advocacy Network and our 2022 STARS sponsors Lilly, Bayer, BMS, and Genentech for supporting this event!
This presentation was given on April 6, 2022, by Janet Freeman-Daily (a lung cancer patient research advocate) at the IASLC 2022 World Conference on Lung Cancer (#WCLC22) in Vienna, Austria during the “Social Media + Communications Workshop.”
Lung cancer patient advocates share purpose, laughter, and tears. On #World Lung Cancer Day, I celebrate efforts to improve outcomes & quality of life for people living with lung cancer. Most of us have/had lung cancer. Many have died. Still, we persist because … we see how we make a difference. #LCSM #WLCD
Below I’ve listed several large, established nonprofit organizations engaged in some aspect of lung cancer patient advocacy. All provide medically validated information about lung cancer, offer patient supports, and/or fund lung cancer research. Many individual patients (like me) and smaller nonprofits are also engaged in aspects of lung cancer patient advocacy.
In early June, the American Society of Clinical Oncology held its 2022 Annual Meeting (#ASCO22) in Chicago. This was the first in-person annual meeting since the pandemic began. While attendance was smaller than usual, McCormick Place (the largest convention center in North America) still hosted 30,000 oncology-related clinicians, researchers, healthcare professionals, patients, and advocates from all over the world.
To address the risk of COVID-19 transmission, attendees were required to prove they were fully vaccinated against COVID-19. Attendees also were required to have a negative COVID-19 test, and COVID tests were readily available during the conference. Masking was recommended – “ASCO expects all attendees to be masked indoors at our meeting when not eating, drinking, or presenting.”
I am a cancer research advocate living with incurable lung cancer for over eleven years. I started attending ASCO Annual Meetings in 2014. It’s wonderful to gather with other cancer patient advocates, network with oncology professionals, and learn about the newest research for my disease. I would have loved to attend in person this year, but I didn’t. I chose to attend virtually during the pandemic because my radiation-scarred lungs are prone to infection (I’ve had pneumonia more than once since my diagnosis), and lung cancer patients are at increased risk of death from COVID-19. However, I had a window into the happenings at McCormick Place via the #ASCO22 hashtag on Twitter, as well as texts and messaging from friends who were there.
Many attendees tweeted pictures of colleagues reunited after a long, trying absence. The pandemic has been especially tough on medical professionals. They needed the joy that reconnection brings. I don’t begrudge them that.
However, those images generated a different emotion for me. After speaking with several friends in the lung cancer patient advocate community, I’ve learned I’m not alone in my feelings.
I’m pissed that the ASCO community appears to have given so little value to the safety of people who have cancer. Here’s why.
RISK OF COVID-19 TRANSMISSION AT #ASCO22 WAS KNOWN BEFOREHAND TO BE HIGH
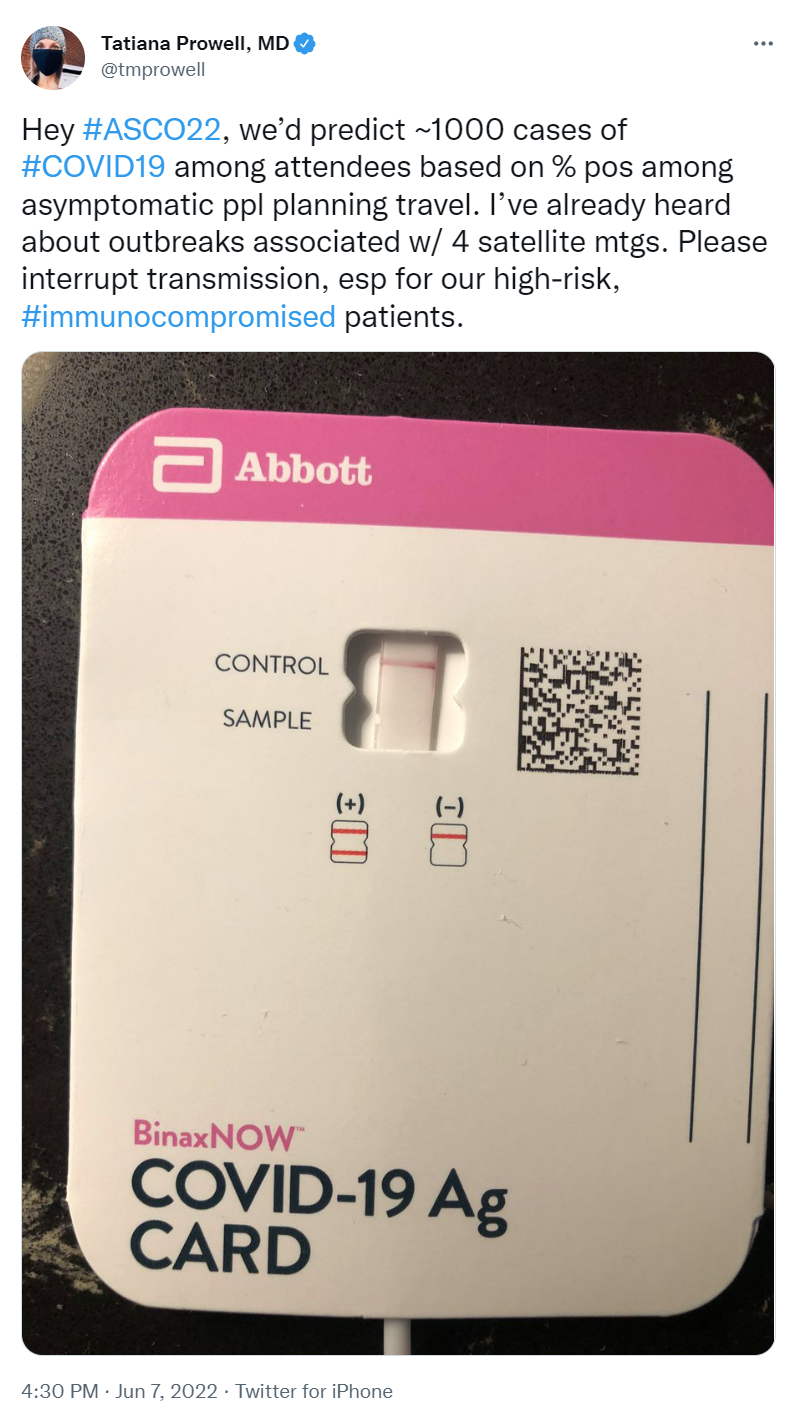
COVID-19 transmission was deemed high in Chicago by the city’s COVID Dashboard in the weeks leading up to #ASCO22. Omicron variants were on the rise and deemed very transmissible. With tens of thousands in attendance, chances of encountering someone infected with COVID were NOT low. Although omicron symptoms seem generally less severe, people are still dying from it–especially people with underlying conditions, like cancer. Others have lingering side effects.
Several medical professionals who attended the smaller 2022 American Association of Cancer Research (#AACR22) Annual Meeting in New Orleans last April tested positive for COVID-19 a few days after the meeting. Masks were not required at AACR, and few masks were seen in surrounding hotels, restaurants, and public transportation. By the start date of the much larger ASCO meeting two months later, community transmission of COVID was much higher. The likelihood someone at #ASCO22 would become infected was a virtual given.
MASKS WERE EXPECTED, BUT NOT REQUIRED
While ASCO expected masks to be worn, masking was not required nor enforced. On the second day of the conference, a tweet observed that perhaps 50% of attendees were wearing masks. Other tweets showed some attendees gathered for selfies and group pictures in session rooms and hallways wearing no masks. Others reported people at ancillary events and hosted parties that included food were frequently unmasked.
ONLY ONE COVID-19 TEST WAS REQUIRED, AND RESULTS WERE NOT CHECKED
ASCO 2022 required a COVID-19 test “within 48 hours of the time they entered any of the session rooms or exhibit hall.” This allowed international attendees with long flights to test after they arrived at McCormick Place. However, testing relied on the honor system: no one verified nor recorded test results. Both rapid and PCR tests were readily available throughout the conference for those who wished to test again, but no system was available for posting results. One doctor who planned to attend tested negative for COVID the day before travel. To be extra safe, they tested just before leaving for the airport. That second test was positive. As a result, she chose not to attend the conference.
It’s unlikely everyone was equally diligent with testing. How many people arrived at the conference unknowingly positive?
ONCOLOGY PROFESSIONALS, YOUR PATIENTS WANT YOU TO SET THE EXAMPLE
Oncology is a medical field that’s evidence based and highly dependent on data. Good results demonstrated in clinical trial data are essential to getting new cancer drugs approved by regulators and available to patients. One would think oncology professionals would be the first to follow the data when it comes to protecting their patients from COVID-19. People who have cancer expect our doctors, nurses, and other clinical professionals to set and maintain a high bar.
So many patient advocates typically attend ASCO that the meeting offers a Patient Advocate Lounge as well as patient-focused programs. Many of these advocates have active cancer. Before the meeting, both patient advocates and doctors pleaded with ASCO to make masking a requirement to reduce the risk of spreading of COVID to patients who attended ASCO, and to healthcare providers at ASCO who would be seeing patients in clinic when they returned home. ASCO refused. The letter has since been taken down, but is mentioned in this article.
Lung cancer patient and research advocate Jill Feldman had the honor of being invited to speak in an ASCO education session. Including patients on ASCO panels is still rare, and Jill takes the responsibility of representing the patient voice seriously. She chose to forego in-person ASCO except for the session in which she was speaking because she had significant COVID anxiety — she’d been hospitalized for the virus last December. She lives near Chicago, so she didn’t have to fly or stay in a hotel. She wore an N95 mask, except for her time on the podium. A tweeted picture of the audience in her session (since deleted) showed many faces and few masks. Despite Jill sharing her anxiety about possible COVID exposure at the end of her talk, some ASCO attendees approached her afterwards to chat without wearing masks.
I am grateful for the oncology professionals who are caring for me. I am glad they feel renewed by their experience at #ASCO22. I appreciate those who were careful to stay masked while at the conference.
Still, I am angry about the apparent disregard for people who have cancer that was demonstrated by ASCO as a community and the oncology profession as a whole. Many #ASCO22 attendees were unmasked while hugging, sitting shoulder-to-shoulder in sessions, chatting while in noisy food courts, catching up over Exhibit Hall lattes, and networking at after-hours parties. I wonder how many of them (or the people they were near) were in clinic the next day sharing their ASCO joy and COVID with immunocompromised patients.
A fellow lung cancer advocate and virtual #ASCO22 attendee tweeted her decision not to attend in person. Her choice was widely applauded: in five days, her tweet received almost 2000 likes, 200+ retweets, and dozens of “thank you” responses.
C’mon, ASCO community, you can do better. Cancer patients expect – no, REQUIRE – you to set a high bar. Step up.
The rule of law should be equally applied to all, don’t you think? So, if the only reason to have sex is to create babies and carry them to term so they can have life, liberty, and the pursuit of happiness, and any pregnant person MUST carry the pregnancy to term no matter the impact on the mother’s life,
then …
We must ensure all potential parents are at least as prepared for parenting as adoptive parents are required to be.
These guidelines should help.
1. All males must be sterilized at puberty. No pregnancy can occur without male input.
2. A male can have sterilization reversed ONLY when they prove they:
want to raise children,
have acceptable parenting skills, and
are able to support children in an acceptable home environment.
3. A male may only engage in sex with a person who:
explicitly states in writing that they are willing and able to bear and raise a child with that specific male, and
can prove that they are able to support a child should something happen to the male.
4. Any male who violates these rules will be:
immediately and permanently sterilized,
jailed for 9 months while wearing a pregnancy suit,
required to work in the jail’s diaper service for another 4 years,
for the next 30 years after release from jail, required to work in a minimum-wage job while paying a monthly “standardized offspring support fee” calculated to equal 50% of food, housing, education, daycare, and medical bills for a child with a disabling condition.
I wonder how many men that would leave to run the country?
Today marks 11 years since I was first diagnosed with advanced lung cancer.
Eleven years with the mostly deadly cancer. Imagine that!
When I was diagnosed, my life expectancy was 2 years on the outside, and that was higher than the average because I was relatively young and otherwise healthy. The majority of lung cancer patients died within a year of diagnosis.
Thanks to online patient communities, targeted therapies, biomarker testing, clinical trials, and dedicated clinicians like Dr. Ross Camidge, whose smiling face appears next to mine in this picture, I’m still here. These things, along with additional new treatments like immunotherapy, new biomarkers, lung cancer screening, and ongoing medical research are changing the face of lung cancer. The expected survival of advanced lung cancer patients has risen by several YEARS since I was diagnosed.
Today, I’m grateful. Grateful for the medical research and treatments that have kept me alive with a good quality of life. Grateful for the additional time I’ve had with my family and this amazing universe. Grateful for finding a new purpose as a lung cancer research advocate collaborating on The ROS1ders, IASLC Supportive Training for Advocates on Research and Science (STARS), and other projects. And especially, I’m grateful for the wonderful friends and colleagues I’ve met along the way.
My prayer is that someday ALL people will have ready access to effective treatments and compassionate care for their health conditions, no matter what they look like, where they live, how much money they have, or how others believe they should be treated.
GO2 Foundation for Lung Cancer (with the support of the entire lung cancer community) has submitted an appropriations request of $60M in the FY23 Defense Appropriations Bill with a goal to increase funding for the Department of Defense Lung Cancer Research Program (DOD LCRP) to $60M from its current $20M. The entire lung cancer community is joining forces to make it happen!
It takes only a couple of minutes to make your voice heard. But when all our voices join together, it becomes a ROAR.
Please click the link below and follow the instructions to tell your US Senator & Representatives to support $60 million for federal lung cancer research in 2023. Tell your friends & family. Please share widely on all your social media platforms.
HURRY! The House letter deadline is April 26 and Senate letter deadline is May 12, so don’t wait.
Today Washington’s state-wide mask mandate is gone (though masks are still required in some settings). When you see people still wearing masks, please don’t give us a hard time. You don’t know the health conditions we or people we love may have.
The mask mandate is gone, but the COVID-19 virus is not. Medical research has collected data that shows certain populations are at higher risk of severe or fatal COVID-19 if exposed to it. Older people, especially those over age 80, have less effective immune systems.
Sometimes people are at greater risk because of physical issues. My lungs have been damaged by radiation treatment for lung cancer, and are unable to clear nasties as effectively as they once did. I’ve had pneumonia several times since my cancer diagnosis nearly 11 years ago. Hospital data shows people with some chronic conditions like heart disease and diabetes are more likely to get severely ill if they get the virus.
Some people are at greater risk due to compromised immune systems. Medical treatments like chemotherapy or high-dose steroids impair the immune system. Very young children have immature immune systems.
It’s not a given we’ll get severely sick, but the odds are not in our favor. We’re into risk reduction. Medical data show KN95 and N95 masks reduce the likelihood of catching COVID-19. Our doctors suggest we should wear masks when in public. The CDC recommends we continue to wear masks. More data is needed for those of us at increased risk before we take off our masks.
When you encounter someone wearing a mask, or resistant to indoor dining in restaurants, or unwilling to attend a event with a large group, please be kind.