Thirteen years ago today, I experienced a revival of hope. In mid September 2012, I had learned my cancer had grown despite two different lines of chemotherapy plus radiation. But on this date, the University of Colorado notified me that my tumor tissue tested positive for a gene rearrangement called ROS1, and I was eligible for a clinical trial of the targeted therapy pill crizotinib. I had options again!
Today I’m still on the same daily pill. Cancer research is awesome.
He’s a world famous lung cancer doctor. He’s an expert in my rare type of cancer (ROS1+ lung cancer). He is the person who started the oncology remote second opinion program at University Of Colorado. He is on the scientific advisory board of the nonprofit I cofounded (The ROS1ders). He is a principal investigator on the clinical trial that saved my life. I’m proud to say he is a personal friend.
On Monday September 8 I learned he is also a person living with lung cancer.
I applaud him for going public with his story. It also breaks my heart.
45 years ago today, Mount St. Helens erupted. From my home in Tacoma over 70 miles away, I could hear and feel the blast and see the plume of ash, rock, and hot gases rising into the atmosphere.
Such major blasts of chaotic energy and hot gases produce extensive damage. The explosion darked the skies for miles, extinguished lives, erased forests, and rearranged the landscape. The melted glacial ice generated a lahar that carried away homes, destroyed highway bridges, and clogged shipping lanes. The blast left behind tons upon tons of pulverized rock that continue to cause challenges for communities living downstream–such as clogging their drinking water systems.
Mount St. Helens is now one of the most closely monitored volcanos in the world. Last Saturday at the Cascade Volcano Observatory (CVO) open house I learned about different types of volcanoes, effects of eruptions on living creatures and the earth, how we track and model earthquakes to predict eruptions, understanding lahar flows so we can provide early warnings, and atmospheric influences on that guide ash and volcanic gas distribution. Models for making these predictions depend on data gathered by a variety of sources, such as weather balloons launched by the National Oceanic and Atmospheric Administration (NOAA). We can’t prevent volcanoes from erupting, but we can improve our preparedness and detection abilities so we can help reduce deaths and damage–IF we can learn from history and maintain the will to and funding to do what is necessary.
The posters I’m sharing in this blog were on display at the CVO open house. CVO is part of the Volcano Hazards Program run the by U.S. Geological Survey (USGS), which is under the U.S. Department of the Interior. Many USGS scientists and staff have departed in response to government actions of the past few months. In May the federal government has notified USGS researchers and students that their funds could be frozen and staff could be laid off. Other government cutbacks (such as reduced weather balloon launches) reduce USGS ability to monitor volcano activity, not to mention the U.S. Weather Service’s ability to predict tornadoes and other severe weather.
Despite the devastation, signs of life returned to the desolate blast zone within months, but it will never appear as it did before the eruption. If we don’t actively pursue the objective study of our world, we not only limit our learning about the world we live in, we will become less able to predict impending disasters and protect lives. Guess we’ll just have to adapt when natural disasters strike. If we can.
If anyone is still inclined to think the government’s efforts to delete “DEI” hires are aimed at people hired for reasons other than their skills, consider the case of the Navajo Code Talkers. Pages about them have been removed from DOD websites and replaced with “DEI.”
These Americans had a unique skill that no one else possessed. Their ability to speak in Navajo during WWII created a code that no enemy ever broke. They enabled us to win critical battles during World War II. High-level military leaders said the Allies could not have won those battles without them.
And yet they’ve been cancelled. Erased. Told they were only hired because they looked different than the majority population in the US during WWII, before the civil rights movement even existed. They accomplished it all despite the prejudice against them.
Where are all the objections to “cancel culture” now? Crickets.
I am ashamed of the way our government is erasing genuine accomplishments by people who don’t look like them or fit their definition of warfighter.
I’ve chosen a conservative media site for the supporting news article to show this isn’t a deception by liberal media. The image on this blog comes from this article.
I’ve been living with and communicating about lung cancer for over 13 years. Since 2011 (the year I was diagnosed) I’ve been active in one or more online lung cancer patient groups. Since 2012, I’ve been blogging and on social media, connecting with the lung cancer community and learning/sharing developments in cancer research. In 2013, I cofounded #LCSM (lung cancer social media) Chat on Twitter and became a co-moderator of its weekly chats. As an active lung cancer patient research advocate, I’ve presented at national and international oncology conferences about using social media in the lung cancer community to improve education, clinical trials., and patient care.
Nowadays I spend most of my social media time in the private “ROS1 Positive (ROS1+) Cancer” Facebook group I cofounded (my ROS1+ cancer is a rarer form of lung cancer) and related online accounts. I know there are data security risks in sharing my cancer journey on public and private social media platforms, but it’s one of the most effective ways to reach other people who are living with lung cancer, especially for rarer subtypes.
All of that is to give you some background about my participation in social media. I’ve been very active online. I don’t sift through random posts about celebrities or debates about news events, but I have been known to spend hours online following developments in cancer research, posts from people attending oncology conferences, and discussions about cancer care from the patient perspective.
I used to do a lot of my research and outreach on Twitter. But due to evolving policies, algorithms, and accounts on X, I now spend almost no time on that platform. The Elon era substantially reduced its usefulness for this lung cancer patient advocate. I’ll try to explain why.
While cancer social media has always had to contend with medical misinformation, it became significantly worse on X after moderation was cut back. I’ve also seen a dramatic increase in hateful comments, personal attacks, and anti-science sentiment. I don’t want to waste my time reading that stuff while trying to find the content I value.
A blue checkmark on an account used to mean that account was owned by a validated organization, agency, or individual that had significant public impact. Patients could distinguish which accounts shared trusted, evidenced-based medical information . Now anyone can buy a blue checkmark, impersonate whoever they want, and spread medical disinformation that is not helpful or safe. While not all patients are successfully treated, the survival rate for lung cancer has increased significantly over the past decade. I’m not the only metastatic lung cancer patient who has survived for more than 10 years thanks to newer treatments like targeted therapies and immune checkpoint inhibitors. Yet I know people who died because they decided to forego an evidenced-based new cancer treatment in favor of some “cure” they found online that had only a few anonymous anecdotes to support it.
When you blocked someone on Twitter, you could no longer see them and they could no longer see you. Now when you block someone on X for malicious behavior, they can still see your posts. I prefer to have more control over who sees my content.
The platform terminated its free API (Application Programming Interface). This disrupted a lot of applications and websites that patient advocates and others used to interact with the platform and archive material from online chats. I have to spend more time to accomplish less.
My X feed used to be filled with content from people I chose to follow. Now it’s filled with ads and people I never chose to follow that don’t interest me in the slightest. I can’t find the content I want, and those who follow me don’t see the content I generate. The only way I can find useful cancer-related content is by using hashtags like #lcsm, but even hashtag-curated content is greatly reduced because so many members of the cancer community have stopped posting on the platform.
As of today, any content posted on X can be used to feed AI engines. While I’ve always known my posts on Twitter/X were publicly visible, it does bother me that the platform would deliberately hijack my content for their own uses without any acknowledgment or compensation.
So, there it is. I want to make a difference in the cancer space, and I have a limited amount of time and energy available to do it. Wading through uncurated content, hostile posts, and medical misinformation isn’t how I want to spend my days.
It’s sad to see the era of Twitter cancer communities end. Twitter was the one place where all stakeholders–patients, caregivers, advocates, clinicians, academic cancer centers, researchers, government agencies, industry, and the general public–could meet and exchange ideas on something that had life-and-death implications for so many (lung cancer is the #1 cancer killer). I hope someday another platform will attract enough participants to once again enable discussions across silos.
Lung cancer research gives patients hope, time with loved ones, and better quality of life. Ten years ago today, I entered a targeted therapy clinical trial for my ROS1+ lung cancer, taking an oral drug called crizotinib (trade name Xalkori). I’m still taking it (it’s now approved by the FDA and in many other countries) and have had no evidence of disease since I started it. Pretty amazing, since I had been given an expiration date of 2 years at the outside for my metastatic non-small cell lung cancer.
In early June, the American Society of Clinical Oncology held its 2022 Annual Meeting (#ASCO22) in Chicago. This was the first in-person annual meeting since the pandemic began. While attendance was smaller than usual, McCormick Place (the largest convention center in North America) still hosted 30,000 oncology-related clinicians, researchers, healthcare professionals, patients, and advocates from all over the world.
To address the risk of COVID-19 transmission, attendees were required to prove they were fully vaccinated against COVID-19. Attendees also were required to have a negative COVID-19 test, and COVID tests were readily available during the conference. Masking was recommended – “ASCO expects all attendees to be masked indoors at our meeting when not eating, drinking, or presenting.”
I am a cancer research advocate living with incurable lung cancer for over eleven years. I started attending ASCO Annual Meetings in 2014. It’s wonderful to gather with other cancer patient advocates, network with oncology professionals, and learn about the newest research for my disease. I would have loved to attend in person this year, but I didn’t. I chose to attend virtually during the pandemic because my radiation-scarred lungs are prone to infection (I’ve had pneumonia more than once since my diagnosis), and lung cancer patients are at increased risk of death from COVID-19. However, I had a window into the happenings at McCormick Place via the #ASCO22 hashtag on Twitter, as well as texts and messaging from friends who were there.
Many attendees tweeted pictures of colleagues reunited after a long, trying absence. The pandemic has been especially tough on medical professionals. They needed the joy that reconnection brings. I don’t begrudge them that.
However, those images generated a different emotion for me. After speaking with several friends in the lung cancer patient advocate community, I’ve learned I’m not alone in my feelings.
I’m pissed that the ASCO community appears to have given so little value to the safety of people who have cancer. Here’s why.
RISK OF COVID-19 TRANSMISSION AT #ASCO22 WAS KNOWN BEFOREHAND TO BE HIGH
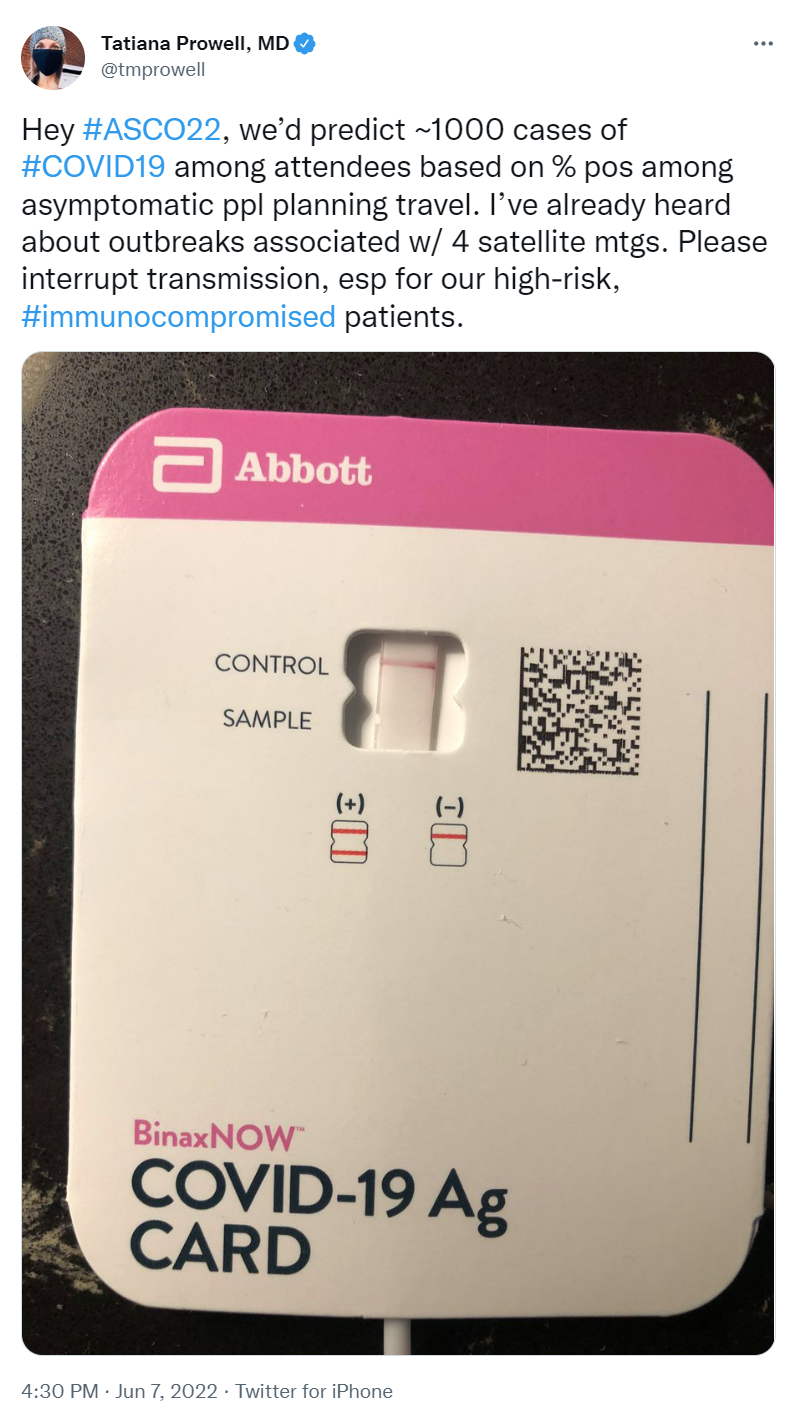
COVID-19 transmission was deemed high in Chicago by the city’s COVID Dashboard in the weeks leading up to #ASCO22. Omicron variants were on the rise and deemed very transmissible. With tens of thousands in attendance, chances of encountering someone infected with COVID were NOT low. Although omicron symptoms seem generally less severe, people are still dying from it–especially people with underlying conditions, like cancer. Others have lingering side effects.
Several medical professionals who attended the smaller 2022 American Association of Cancer Research (#AACR22) Annual Meeting in New Orleans last April tested positive for COVID-19 a few days after the meeting. Masks were not required at AACR, and few masks were seen in surrounding hotels, restaurants, and public transportation. By the start date of the much larger ASCO meeting two months later, community transmission of COVID was much higher. The likelihood someone at #ASCO22 would become infected was a virtual given.
MASKS WERE EXPECTED, BUT NOT REQUIRED
While ASCO expected masks to be worn, masking was not required nor enforced. On the second day of the conference, a tweet observed that perhaps 50% of attendees were wearing masks. Other tweets showed some attendees gathered for selfies and group pictures in session rooms and hallways wearing no masks. Others reported people at ancillary events and hosted parties that included food were frequently unmasked.
ONLY ONE COVID-19 TEST WAS REQUIRED, AND RESULTS WERE NOT CHECKED
ASCO 2022 required a COVID-19 test “within 48 hours of the time they entered any of the session rooms or exhibit hall.” This allowed international attendees with long flights to test after they arrived at McCormick Place. However, testing relied on the honor system: no one verified nor recorded test results. Both rapid and PCR tests were readily available throughout the conference for those who wished to test again, but no system was available for posting results. One doctor who planned to attend tested negative for COVID the day before travel. To be extra safe, they tested just before leaving for the airport. That second test was positive. As a result, she chose not to attend the conference.
It’s unlikely everyone was equally diligent with testing. How many people arrived at the conference unknowingly positive?
ONCOLOGY PROFESSIONALS, YOUR PATIENTS WANT YOU TO SET THE EXAMPLE
Oncology is a medical field that’s evidence based and highly dependent on data. Good results demonstrated in clinical trial data are essential to getting new cancer drugs approved by regulators and available to patients. One would think oncology professionals would be the first to follow the data when it comes to protecting their patients from COVID-19. People who have cancer expect our doctors, nurses, and other clinical professionals to set and maintain a high bar.
So many patient advocates typically attend ASCO that the meeting offers a Patient Advocate Lounge as well as patient-focused programs. Many of these advocates have active cancer. Before the meeting, both patient advocates and doctors pleaded with ASCO to make masking a requirement to reduce the risk of spreading of COVID to patients who attended ASCO, and to healthcare providers at ASCO who would be seeing patients in clinic when they returned home. ASCO refused. The letter has since been taken down, but is mentioned in this article.
Lung cancer patient and research advocate Jill Feldman had the honor of being invited to speak in an ASCO education session. Including patients on ASCO panels is still rare, and Jill takes the responsibility of representing the patient voice seriously. She chose to forego in-person ASCO except for the session in which she was speaking because she had significant COVID anxiety — she’d been hospitalized for the virus last December. She lives near Chicago, so she didn’t have to fly or stay in a hotel. She wore an N95 mask, except for her time on the podium. A tweeted picture of the audience in her session (since deleted) showed many faces and few masks. Despite Jill sharing her anxiety about possible COVID exposure at the end of her talk, some ASCO attendees approached her afterwards to chat without wearing masks.
I am grateful for the oncology professionals who are caring for me. I am glad they feel renewed by their experience at #ASCO22. I appreciate those who were careful to stay masked while at the conference.
Still, I am angry about the apparent disregard for people who have cancer that was demonstrated by ASCO as a community and the oncology profession as a whole. Many #ASCO22 attendees were unmasked while hugging, sitting shoulder-to-shoulder in sessions, chatting while in noisy food courts, catching up over Exhibit Hall lattes, and networking at after-hours parties. I wonder how many of them (or the people they were near) were in clinic the next day sharing their ASCO joy and COVID with immunocompromised patients.
A fellow lung cancer advocate and virtual #ASCO22 attendee tweeted her decision not to attend in person. Her choice was widely applauded: in five days, her tweet received almost 2000 likes, 200+ retweets, and dozens of “thank you” responses.
C’mon, ASCO community, you can do better. Cancer patients expect – no, REQUIRE – you to set a high bar. Step up.
Today marks 11 years since I was first diagnosed with advanced lung cancer.
Eleven years with the mostly deadly cancer. Imagine that!
When I was diagnosed, my life expectancy was 2 years on the outside, and that was higher than the average because I was relatively young and otherwise healthy. The majority of lung cancer patients died within a year of diagnosis.
Thanks to online patient communities, targeted therapies, biomarker testing, clinical trials, and dedicated clinicians like Dr. Ross Camidge, whose smiling face appears next to mine in this picture, I’m still here. These things, along with additional new treatments like immunotherapy, new biomarkers, lung cancer screening, and ongoing medical research are changing the face of lung cancer. The expected survival of advanced lung cancer patients has risen by several YEARS since I was diagnosed.
Today, I’m grateful. Grateful for the medical research and treatments that have kept me alive with a good quality of life. Grateful for the additional time I’ve had with my family and this amazing universe. Grateful for finding a new purpose as a lung cancer research advocate collaborating on The ROS1ders, IASLC Supportive Training for Advocates on Research and Science (STARS), and other projects. And especially, I’m grateful for the wonderful friends and colleagues I’ve met along the way.
My prayer is that someday ALL people will have ready access to effective treatments and compassionate care for their health conditions, no matter what they look like, where they live, how much money they have, or how others believe they should be treated.
In May 2011—over 10 years ago–I was diagnosed with advanced lung cancer. At that time, chemo and radiation were the only approved first line treatments for advanced or metastatic lung cancer. Despite undergoing chemo and radiation (twice), my cancer spread to my other lung and became metastatic. I was not inspired by the five-year survival rate for metastatic lung cancer patients back then—it was around 2%.
However, in early 2011 a small clinical trial for a targeted therapy pill called crizotinib (trade name Xalkori) had begun for ROS1 positive (ROS1+) lung cancer. This cancer is driven by an acquired alteration in the ROS1 gene. This pill that sounded like an alien seemed to inhibit ROS1+ cancer in about 80% of people in the trial. That was amazingly effective for a cancer drug!
In the fall of 2012, I arranged to have my tumor tissue tested and discovered my cancer was ROS1+. I mentioned the clinical trial option to my oncologist, and he recommended I join the trial (even though it required travel) because the preliminary trial results looked promising. All he could offer me otherwise was a lifetime on a chemo that didn’t make me feel much like living.
I enrolled in the trial in Denver, Colorado—over 1000 away from home—on November 6, 2012, and hoped for the best.
I’m still here thanks to research. Today marks 9 years since I took my first crizotinib pill. I have had No Evidence of Disease (meaning no cancer shows up on any scans) ever since. Although I’m incredibly grateful to be alive and have a relatively normal life with tolerable side effects, I’m always looking over my shoulder. No one can tell me if I’m cured, because few others have been on the drug this long. Most patients find their cancer eventually becomes resistant to crizotinib and their cancer resumes growing. The population of ROS1+ patients is relatively small (only 1-2% of lung cancer patients have ROS1+ cancer), so research on our type of cancer is sparse. We have some clinical trials in process, but no second line targeted therapy has yet been shown effective enough to obtain any government approval.
That’s why Lisa Goldman, Tori Tomalia (may she rest in peace) and I–all people who had ROS1+ lung cancer–decided to do something about it. In the spring of 2015 we created a Facebook group for patients and caregivers dealing with ROS1+ cancer, and eventually formed a nonprofit known as The ROS1ders. Our mission is to improve outcomes for all ROS1+ cancers through community, education, and research. We have almost 800 members spanning 30+ countries, and are considered experts in our disease by some of the top oncologists in the world. We’ve already helped create new models of ROS1 cancer that researchers have used in published research.
We’re now planning a research roundtable in December to explore ways to collect real-world data on ROS1+ cancers, and will be hosting a ROS1 Shark Tank event next spring that will award two $50,000 seed grants for new ROS1 projects. We’re aiming to raise $100,000 this year to fund our work.
Cancer research advocacy is my passion. I’m able to use my skills and time to help make a difference for hundreds of other people living with ROS1+ cancers. It’s a purpose that keeps me going despite the ever-present specter of potential recurrence.
I know there are many worthy charities asking for money this time of year. Any small amount you can give will help accelerate research for hundreds of ROS1ders worldwide who, like me, are dying for more treatment options.
Many of my friends who have lung cancer take targeted therapy pills. Mine costs $17K per month when not covered by insurance. Some drugs cost even more.
Unfortunately, most all patients who take targeted therapy pills see their cancer eventually start to grow again. These patients often must change to a different anti-cancer therapy. When a patient has to change therapies, they may be left with unused medications.
Patients on expensive medications HATE to throw out their cancer drugs when those same drugs might help someone else live longer or more comfortably.
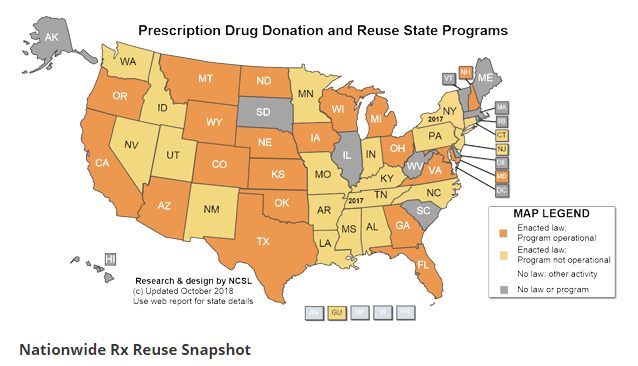
Some US states will allow “prescription reuse” — unopened cancer drugs can be donated for use by a different patient. As the map shows, state laws on this subject vary significantly, and not all states that have enacted prescription reuse laws have operational programs that enable reuse.
Why isn’t this easier? Why can’t I just drop off my unused pills at a pharmacy and know they’ll get to someone who really needs them but can’t afford them?
If you wish to donate unneeded cancer drugs, check with a local pharmacy or prescriber for practical advice on what may work in your situation, in your state. If your state has no operating program, contact your state legislators.
What a great opportunity for patient advocacy to make a difference!