Once a person is medically diagnosed with having metastatic cancer (cancer that has spread to other organs), some people accuse that person of lying when the person says they didn’t know they had cancer. Because some cancers might grow for years before spreading to other organs, people think the person with cancer would had to have known they had it.
After more than a decade of living with metastatic lung cancer and serving as a patient research advocate, I have seen plenty evidence this need not be the case. Here are some important factoids about lung cancer that also hold true for other types of cancer:
1. Not all cancers have symptoms while they are growing. Lung cancer rarely has symptoms until it has spread to other organs. Lungs don’t have nerves to say “ouch!” when a tumor is growing. For this reason, the vast majority of lung cancers were not detected until the cancer had spread elsewhere before the advent of lung cancer screening. But not everyone is eligible for lung cancer screening. Screening is limited to people who are at increased risk of developing cancer and who can benefit from treatment–this is to minimize the risk of overdiagnosing and treating people who don’t need cancer treatment.
2. Not all cancer grows at the same rate. When I was diagnosed in 2011, I was told my non-small lung cancer did not grow fast and would have taken years to create the 2.5 inch tumor in my lung. I had months of combined chemo and radiation treatments designed to cure me of my cancer. Yet three months after a CT scan said my tumors were almost gone, I had grown a new three-inch tumor at the base of my neck. Some types of cancers are much more aggressive than others.
3. Best practice medical care might not be looking for cancer. Another friend (age in mid-20s) reported shortness of breath when running. Because they were so young, their doctor took a conservative approach to treatment. My friend was treated for allergies, and then pneumonia. By the time doctors prescribed a CT scan, the lung cancer had spread to several other organs. You can’t find something when you’re not looking for it.
4. Not all cancer is detectable with current technology. A friend who had lung cancer had a brain scan using magnetic resonance imaging (MRI). The scan showed their brain was clear of cancer. Three weeks later they began leaning slightly to one side while walking. A second brain MRI scan found sizeable tumors in their brain that didn’t show up just a few week earlier. The seeds of those tumors likely existed when they had the first brain scan, but scan technology is not sensitive enough to detect cancer that small.
My take-away message Don’t assume that someone must have known they had cancer just because it had spread to other organs by the time it was officially diagnosed. Many people honestly had no idea they had cancer before they were diagnosed. I didn’t.
45 years ago today, Mount St. Helens erupted. From my home in Tacoma over 70 miles away, I could hear and feel the blast and see the plume of ash, rock, and hot gases rising into the atmosphere.
Such major blasts of chaotic energy and hot gases produce extensive damage. The explosion darked the skies for miles, extinguished lives, erased forests, and rearranged the landscape. The melted glacial ice generated a lahar that carried away homes, destroyed highway bridges, and clogged shipping lanes. The blast left behind tons upon tons of pulverized rock that continue to cause challenges for communities living downstream–such as clogging their drinking water systems.
Mount St. Helens is now one of the most closely monitored volcanos in the world. Last Saturday at the Cascade Volcano Observatory (CVO) open house I learned about different types of volcanoes, effects of eruptions on living creatures and the earth, how we track and model earthquakes to predict eruptions, understanding lahar flows so we can provide early warnings, and atmospheric influences on that guide ash and volcanic gas distribution. Models for making these predictions depend on data gathered by a variety of sources, such as weather balloons launched by the National Oceanic and Atmospheric Administration (NOAA). We can’t prevent volcanoes from erupting, but we can improve our preparedness and detection abilities so we can help reduce deaths and damage–IF we can learn from history and maintain the will to and funding to do what is necessary.
The posters I’m sharing in this blog were on display at the CVO open house. CVO is part of the Volcano Hazards Program run the by U.S. Geological Survey (USGS), which is under the U.S. Department of the Interior. Many USGS scientists and staff have departed in response to government actions of the past few months. In May the federal government has notified USGS researchers and students that their funds could be frozen and staff could be laid off. Other government cutbacks (such as reduced weather balloon launches) reduce USGS ability to monitor volcano activity, not to mention the U.S. Weather Service’s ability to predict tornadoes and other severe weather.
Despite the devastation, signs of life returned to the desolate blast zone within months, but it will never appear as it did before the eruption. If we don’t actively pursue the objective study of our world, we not only limit our learning about the world we live in, we will become less able to predict impending disasters and protect lives. Guess we’ll just have to adapt when natural disasters strike. If we can.
I’ve been thinking about why some people don’t trust medical science and doctors in the US (and, increasingly, globally).
I’m not talking about issues with the medical system like ethical lapses, insurance snafus, cost, poor communications, malpractice, politicization, etc. I want to talk about issues with science.
I think a major source of distrust in medical science lies in the fact that no two human bodies are exactly alike–not even two identical twins. Stay with me on this one–it takes a while to explain.
For some medical procedures, like setting a broken bone, results are pretty predictable for the vast majority of people. However, when it comes to more complicated health issues like cancer and viruses, it’s less certain that medical science can generate specific results due to variations in the human body, nuances in the disease, and the fact that we don’t know everything about how the body or the disease works. (I’ve got 13 years as a cancer patient to support me on this).
The scientific process of discovery is the same in all areas of science, but the level of evidence available and predictability of results can vary depending on what’s being studied. In the engineering world where I was trained, once a physical law (e.g., the behavior of gravity on earth) has been confirmed by many observers, one can rely on it to remain true–at least until new data suggests the law may need to be revised.
The same is not true in medical science.
In medical science (particularly in drug development), a response to treatment in one person does not guarantee the same response will occur in another person who has the same condition. A person’s response can vary due to differences in the body, the environment, other health issues, or even the treatment process. This is why anecdotal evidence is not considered reliable evidence in medical science (although an individual response might indicate something is worth studying). A treatment must produce a similar response in many people to be considered effective–and even then, it may be effective only in people with certain characteristics. Based on decades of cancer research and treatment, claims of “This cancer treatment is guaranteed to work for EVERYBODY!” should generate significant skepticism.
If a hundred studies in engineering produce the same result, we trust the result will be true for all future studies. However, if a medical treatment is effective for 100 people, it still might not be effective for the 101st person. In the case of viruses (which mutate and may have as yet unknown effects on the body), medical evidence can tell you whether a vaccine can reduce your risk of getting infected/sick/dying from the virus, but it’s rare to get exactly the same results for all people.
People want science to be absolutely true, like engineering. When you turn on your stove, you trust it will generate heat for cooking. If it doesn’t work, it’s the machine’s fault, not the science.
But in medicine, the thinking is different. “The doctor said this treatment could keep me from getting sick. I still got sick. The treatment didn’t work, the doctor doesn’t know what they are talking about, the science is bad.”
Perhaps the lack of certainty makes medical science untrustworthy to some. And therefore “science” itself is bad.
Please join #LCSM Chat and other Twitter cancer hashtag communities as we discuss “The Hows and Whys of Cancer Research Advocacy” on Twitter Thursday, May 6th, at 5 pm Pacific (8 pm Eastern). Join us to learn how cancer research advocates bring value to research!
Remember, the IASLC STARS Program is accepting applications for 2021 Patient Research Advocates through May 10! STARS aims to help lung cancer patient advocates evolve into research advocates. https://www.iaslc.org/patient-advocacy/stars
The number of new cases is up more than 20 percent from 2 weeks ago
The number of hospitalizations has increased by 21 percent
The number of deaths has jumped 39 percent, with the United States surpassing 3,000 deaths in 1 day for the first time
On December 11, the United States Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for the first SARS-CoV-2 mRNA vaccine, BNT162b2, manufactured by the pharmaceutical giant, Pfizer. For a description of how mRNA vaccines work, please check our last update available here. The New York times reported that large-scale manufacturing and distribution of vaccines has already begun, with the first dosing to start on December 14, 2020. This huge milestone is a positive step towards fighting the COVID-19 pandemic. However, it is important to keep in mind that it will take a considerable amount of time before the entire US population is either vaccinated or immune to COVID-19 through natural infection. With the year-end holidays around the corner and an anticipated increase in travel, the CDC has extended its travel advisory to include the winter break. We encourage our community members to weigh the risks and benefits of travel during this winter. Thanks to the vaccine, the end of the pandemic may be on the horizon. Till such time, maintaining public health measures such as masking, handwashing, social distancing, and minimizing non-essential travel are our best bets for protection.
How was the Pfizer vaccine approved?
The vaccine was approved based on a randomized, double-blind Phase 2/3 clinical trial. A total of 43,548 participants (older than 16 years) received either two doses of the vaccine or a placebo injection three weeks apart. Participants were followed for safety and for the development of symptomatic COVID-19 for approximately 2 months. Eight participants in the vaccine group developed symptomatic COVID-19, whereas 162 participants in the placebo group developed symptomatic COVID-19. The vaccine was found to be 95% effective in preventing severe COVID-19 symptoms i.e., for every 100 people who received the vaccine, 95 were protected from developing severe COVID-19.
Is the Pfizer vaccine safe?
Side effects reported by trial participants were generally mild or moderate, and reactions were less common and milder in older adults than in younger adults. Those who received the vaccine had localized reactions at the injection site (pain, redness, swelling) and systemic reactions (e.g., fever, headache, muscle ache) at higher rates than placebo recipients, with more reactions following the second dose. Severe fatigue was observed in approximately 4% of vaccine recipients. However, this rate of severe fatigue is also lower than that observed in recipients of approved influenza vaccines for older adults. Serious side effects were similar in both the vaccine and placebo groups (0.6% and 0.5%, respectively).
It is important to keep in mind that we do not have long-term follow-up data from this clinical trial. Sometimes, side effects may show up after months of follow-up. Also, vaccination began in the United Kingdom last week. Two individuals with a history of severe allergic reactions were reported to have had a severe reaction to the vaccine. These individuals carried an EpiPen and use of the pen was sufficient to counteract the allergic reaction. It is anticipated that these reactions will be very rare given that such safety issues were not seen in the large clinical trial. The public health benefits of distributing this vaccine still far outweigh any perceived risks.
What is not known about the Pfizer vaccine?
We do not know whether the vaccine will be effective for more than 2 months, because participants have only been followed for 2 months so far. However, additional data continues to be gathered.
Children (less than 16 years of age), pregnant women, and immunocompromised patients (such as those who have received cell-based therapies or chemotherapy for their cancer) were not included in the study. We do not know if the virus will be safe (in children and pregnant women) or effective (in immunocompromised patients who may not mount an immune response) in the groups excluded from the clinical trial.
The vaccine involves two doses given three weeks apart. The first dose “primes” the immune system to respond while the second dose “boosts” that response. If someone misses the second dose, we do not know whether the vaccine will still be effective.
We don’t yet know whether the vaccine will prevent the recipient from getting infected or from spreading COVID-19. Again, we need more data. We’ll need to continue practicing public health measures such as masking and social distancing even after receiving the vaccine, at least in the near term.
When will I receive the vaccine?
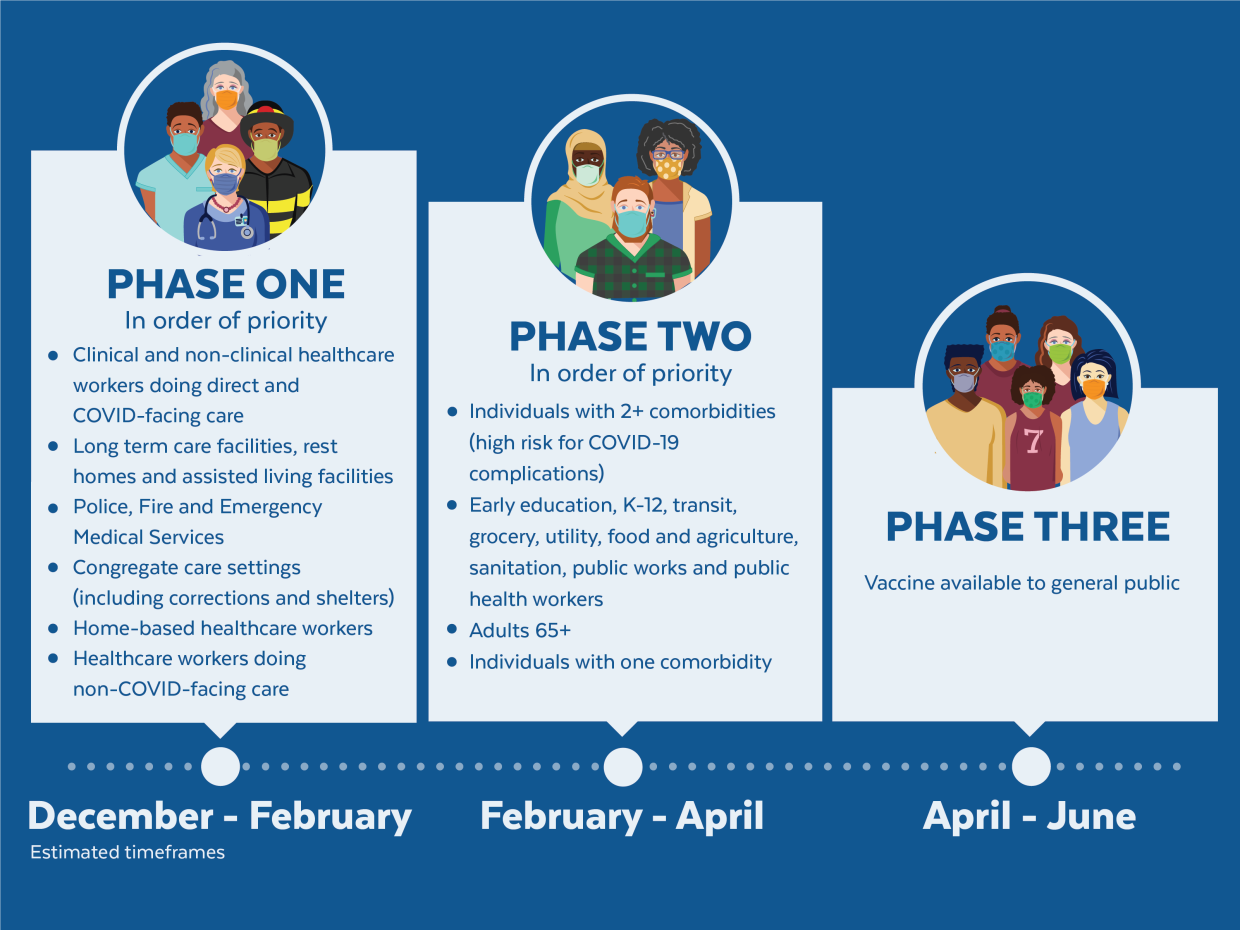
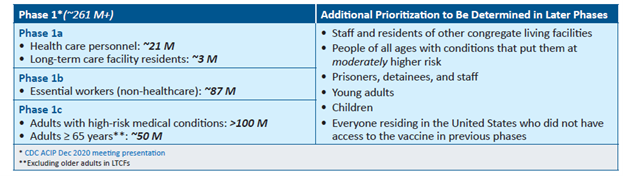
The United States is adopting a phased approach to roll out large-scale vaccination. The phased approach prioritizes the most essential and the most vulnerable of our population as the first recipients of the vaccine, given the initial limited supply of vaccines. The following figure shows how the state of Massachusetts will use the phased approach for distributing vaccines. It is anticipated that patients with lung cancer will receive vaccines in Phase 1 or 2.
As of December 2020, the Advisory Committee on Immunization Practices (ACIP) recommended that both 1) health care personnel and 2) residents of long-term care facilities be offered COVID-19 vaccine in the initial phase of the vaccination program (Phase 1a).
Each state in the United States is likely to have specific vaccination guidelines tailored to their own specific needs. For information specific to your state, please check this link.
An important population for our community is caregivers to patients with lung cancer. If you are the primary caregiver for your loved one, please check your eligibility for receiving the vaccine.
This will be our last update of the year. We wish everyone a safe and peaceful Holiday Season! Please continue to maintain social distancing, wash hands, mask, and minimize non-essential travel. See you in 2021!
We are at a critical moment in the ongoing COVID-19 pandemic. New cases are rapidly escalating throughout the country, and we are positioned to see explosive growth as people travel and gather to celebrate the Thanksgiving holiday with loved ones. While our understanding of how to treat COVID-19 has grown significantly since the disease first burst onto the scene, deaths continue to mount, with the US now seeing the most daily deaths since May.
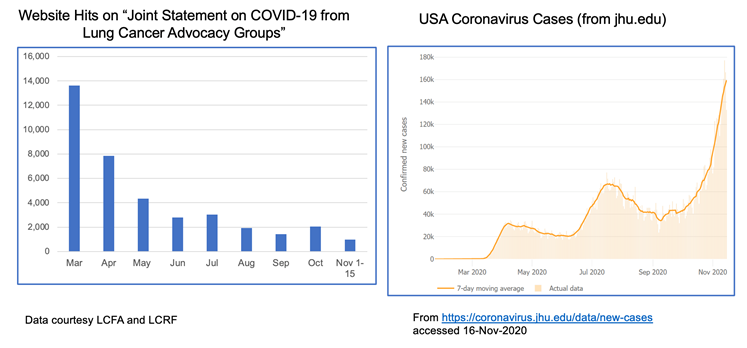
The realities of the current situation are compounded by our collective national fatigue and desire to return to some sense of normalcy. When we look at website hits for these joint statements over time, we see a lot of activity in the spring when COVID-19 was “new,” but those numbers have dropped off substantially through the summer and fall. This stands in stark contrast to the growth of cases through subsequent waves of infection.
The take home message is that we must not let our guard down! Please continue to wear a mask, watch your distance and wash your hands. Our collective actions over the next few weeks CAN make a difference in helping curb the recent surge. We also recognize the importance of balance, particularly for patients with cancer who fear they may not have another Thanksgiving or Christmas. For practical guidance on how to navigate your holidays safely, please refer to this helpful discussion.
Despite the current situation, there is reason for hope. We can now see the light at the end of the tunnel with the recent announcements that both Moderna and Pfizer/BioNTech have developed highly effective COVID-19 vaccines, with others in the pipeline. You can find a comprehensive overview of how vaccine trials work and current vaccine efforts underway here.
Additionally, monoclonal antibody therapies continue to make progress. Eli Lilly recently received Emergency Use Authorization from the FDA for its antibody therapy in recently diagnosed, high-risk patients. Regeneron also received a lot of press when its antibody therapy was used to treat President Trump.
VACCINE FAQS
The development of a new class of mRNA-based vaccines has raised many questions, particularly among the lung cancer community. We have been collecting these questions and will do our best to address them here.
How do mRNA vaccines work?
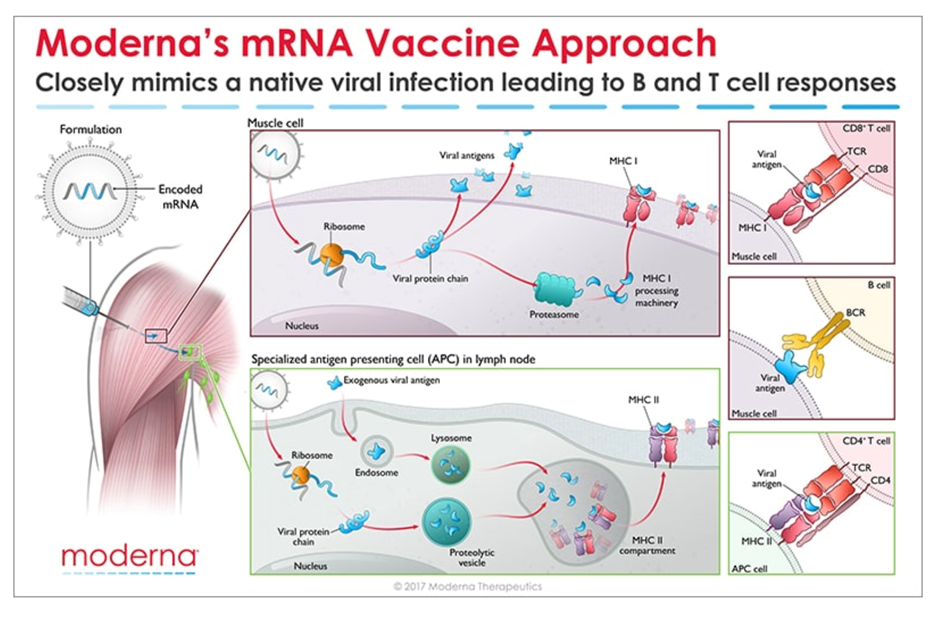
Messenger RNA (mRNA) is the recipe for making a protein. The mRNA gets injected into the body and is taken up by cells that “read the recipe” for making the SARS-CoV-2 spike protein. This is the protein normally expressed as a “crown” on the virus particle and is the part of the virus that binds to the receptor found on cells in the lungs and in other tissues throughout the body. Once these cells take up the mRNA and make the spike protein, they can display pieces of spike on their cell surface to signal the immune cells to become activated. B cells are a type of immune cells that make antibodies that can block virus binding. CD4 T cells support B cells to make antibodies while CD8 T cells can kill virus-infected cells. This is illustrated in the figure below for Moderna’s vaccine (though Pfizer/BioNTech’s vaccine works in the same manner).
How do we know these vaccines are safe?
All new drugs and vaccines go through extensive testing as part of the clinical trials process. (summarized in the NYTimes link above). Both the Moderna and Pfizer/BioNTech vaccines are currently in Phase 3 clinical trials, reporting nearly 95% efficacy and no significant safety issues. It is important to note that these trials have been conducted in thousands of patients. However, no significant safety issues does not mean the vaccines don’t come with some unpleasant side effects which are short-lived. Those effects should not be a reason to avoid the vaccine. Educating healthcare providers on the mRNA technology and ensuring them that the vaccines are safe will be key to a successful rollout.
When will the vaccines be available? Will patients with lung cancer be prioritized?
Based on the safety and efficacy profiles of both vaccines, it is expected that people will start receiving them before the end of the year, perhaps as soon as December 12 in the US. Many national experts are developing guidance for vaccine distribution, with the National Academies issuing a framework that would see healthcare workers, frontline workers and those in high-risk categories being eligible to be vaccinated first. Given that several studies have now reported high mortality rates in patients with lung cancer who contract COVID-19 , it is widely expected that lung cancer patients would be among those first eligible to receive the vaccine in the early stages of rollout.
Should I take the first vaccine available or wait for a later generation one?
As stated earlier, both the Moderna and Pfizer/BioNTech vaccines are highly effective with a strong safety profile. There have been fears among many that the rush to produce a vaccine would result in compromised safety or efficacy but adherence to standards established by the FDA[A1] and other agencies assures us that these vaccines are safe.
It is important to note that before mRNA vaccines were developed in the fight against COVID-19, they were being developed to help combat cancer. Both Moderna and BioNTech (the company that partnered with Pfizer on its COVID-19 vaccine) have been developing mRNA vaccine technology for some time in the hopes of using this approach to treat various forms of cancer as well as other infectious diseases.
Given the unique threat that COVID-19 presents to the lung cancer community, we strongly encourage you to have a discussion with your doctor about getting the vaccine as soon as it is available to you. As for choosing between these two specific vaccines, the technology is essentially identical. Both require two shots over the course of a few weeks. The differences come down to logistical challenges of ensuring facilities have proper freezers for maintaining the vaccines at the appropriate subzero temperatures.
Until those vaccines gain approval, the current decision will be based on availability of the two mRNA-based vaccines.
It is worth noting that a multi-institutional, NCI-funded grant has been awarded to study antibody responses to SARS-CoV-2 infection in lung cancer patients as compared to healthy people. This effort will try to answer why lung cancer patients seem to have worse outcomes from COVID-19 and will study responses in patients receiving a vaccine compared to those who do not.
UNANSWERED QUESTIONS
Several questions remain about the new mRNA vaccines:
Can these vaccines completely prevent infection, or will they just prevent symptoms from developing?
Can people who receive the vaccine still transmit the virus to others?
How long will any resulting immunity last? Previous results from these types of vaccines in other settings suggest that protection may wane after a year.
More data is needed before we can answer these questions.
FINAL TAKEAWAY
There is no escaping the seriousness of our current national crisis – COVID-19 cases are increasing everywhere and so we must do what we can to protect ourselves and our loved ones a little while longer.
However, hope is on the horizon. We can face 2021 knowing that, through the power of science, this pandemic will eventually come to an end.
The first case of COVID-19 in the USA was reported on 1/20/2020—over 9 months ago. Since then, the country has reported 9,860,558 cases and 237,113 deaths (per Johns Hopkins). As the weather becomes cooler and we spend more time indoors, the number of cases is rapidly accelerating in almost every state.
Given this surge, holiday gatherings and activities present a serious risk for virus transmission. On November 5, 2020, the #LCSM (Lung Cancer Social Media) Chat community on Twitter discussed ways to enjoy and celebrate the holidays safely during the pandemic. Chat participants included lung cancer patients, caregivers, advocates, physicians, and healthcare workers. The chat, which included links to many helpful resources, covered the following topics:
What have we learned over the past 8 months about how COVID-19 is transmitted?
How can people reduce the risk of COVID-19 during outdoor activities?
How can people reduce the risk of COVID-19 when travel is involved? What about travel to or from hot spots?
How safe is it to meet with family and friends who had COVID-19 and recovered?
How can people reduce the risk of COVID-19 for indoor activities (shopping, dining in restaurants, family gatherings, worship services, etc.)?
The post below is shared with permission. It can also be found on the websites of the lung cancer advocacy organizations listed at the end of this blog post.
With the run-up to the US Presidential election now less than two months away, recent weeks have seen a growing national dialog on the potential availability of a SARS-CoV-2 vaccine. In this week’s update, we want to review some basic concepts on vaccines, the clinical trials process for ensuring vaccine safety and provide an update on the current status of the various vaccine candidates currently under development.
(PSA: don’t forget to get your flu shot this year!)
How are vaccines tested?
Everyone feels a great sense of urgency to develop a vaccine for SARS-CoV-2 so we can think about returning to some degree of “normalcy” in our daily lives. A concerted global effort is currently underway not only to develop a safe and effective vaccine but to develop other treatments as well (including so called monoclonal antibodies as well as novel antiviral treatments). In the US, the administration has developed what it refers to as “Operation Warp Speed” to try to accelerate vaccine development.
Without getting into a political debate, we want to offer a brief overview of what goes into getting a vaccine approved. Specifically, once a candidate vaccine is identified, its safety and efficacy (how well it works) must be validated through a rigorous clinical trials process as shown in the schematic below:
For a great overview of how vaccines are developed, the different types of vaccines, how they are tested and the status of current efforts to develop a SARS-CoV-2 vaccine, we refer you to an excellent resource put together by The New York Times.
Politics aside, the scientific community must ensure any potential vaccine is both safe AND effective before it is approved and administered to the public. Past experience with the development of SARS and MERS (Middle-Eastern Respiratory Syndrome) vaccines has taught us that coronavirus vaccines need thorough testing. A recent incident that occurred during the Phase 3 clinical trial of AstraZeneca’s vaccine candidate highlights why vaccine safety is paramount. The initial lack of details about the nature of the incident raised concerns about lack of transparency by the drug companies developing these vaccines. In response to mounting pressure, several of the leading contenders have made their protocols public.
Hope on the Horizon
Despite the challenges associated with developing an effective vaccine against SARS-CoV-2, there are several reasons to be hopeful:
The science is advancing at a historic and unprecedented pace. Previously, the fastest vaccine ever made (against mumps) took four years to develop.
We have gone from first identifying a novel virus (SARS-CoV-2) as the cause of COVID-19 (Dec 2019) to having the sequence of the viral genome (Jan 2020) and the pursuit of multiple, compelling vaccine efforts within the span of only six months.
You can find information specific to your state or city or town on your health department’s website:
Directory of state department of health websites
Directory of local health department websites
American Medical Association resources for healthcare providers
The post below is shared with permission. It can also be found on the websites of the lung cancer advocacy organizations listed at the end of this blog post.
With the arrival of September, we are strongly recommending that all eligible patients and caregivers get their annual flu shot this year! Public health experts are particularly concerned about the potential for patients to get infected with both influenza and SARS-CoV-2 this winter. Additionally, since the symptoms for these two viruses are similar, many patients experiencing flu-like symptoms may flood already overtaxed healthcare systems. Many doctors’ offices and pharmacies already have flu shots available. It’s also important to remember that it takes approximately two weeks from receiving the shot to have adequate protection. So please make a plan to get your shot as soon as possible.
Some patients, particularly those on checkpoint inhibitors, may be concerned about whether they can take the flu shot – we always recommend asking your doctor but previous studies suggest that it is safe for patients.
We want to hear from you!
We are interested in knowing what topics we should cover in future updates. Please share your thoughts with us by taking this short (1-2 minute) anonymous survey.
You can find information specific to your state or city or town on your health department’s website:
Directory of state department of health websites
Directory of local health department websites
American Medical Association resources for healthcare providers
The post below is shared with permission. It can also be found on the websites of the lung cancer advocacy organizations listed at the end of this blog post.
—————————
It has been more than 6 months since the first cases of COVID-19 hit the United States. We issued our first update on March 3, a week before the World Health Organization declared a global pandemic on March 11. As of August 24, 2020, cases in the United States continue to rise unabated, with over 5.6 million total cases and 175,000 deaths. Countries in Western Europe that had seen a decrease in case load have recently seen small outbreaks, indicating that community spread continues to be a high possibility.
So we are left to wonder: when can we resume normal activities in our lives?
The straightforward answer to that question is when we have achieved a reasonable level of herd (or community) immunity, which occurs when a high percentage of the community is immune to a disease through vaccination and/or prior illness (natural infection). Herd immunity is critical because it not only prevents the spread of infection but also protects people who may not be able to receive a vaccine (for example, the elderly or the severely immunocompromised in whom the immune system is unable to mount a protective response against the virus).
Epidemiologists are hard at work figuring out what levels of herd immunity will protect us from SARS-CoV-2. Initial models suggested that the percentage of people who need to be immune to the virus to achieve herd immunity was around 70%. However, recent research suggests a lower threshold, on the order of only 40%. It is extremely important to keep in mind that no matter the threshold of immunity required, these estimates are based on mathematical models and not true population-based studies.
Our current level of potential immunity to SARS-CoV-2 (the virus that causes COVID-19) is measured using an antibody assay that detects past exposure to the virus whether or not a person had symptoms of COVID-19. Herd immunity through natural infection may depend on location. For example, levels of herd immunity may be lower in rural areas where people are more spread out than in cities, which are more crowded. Also, older people may be more susceptible to the virus and succumb to the disease, whereas younger people may recover from infections and add to the “pool” of herd immunity. Recent research from a COVID-19 hotspot, New York City, looking at the percentage of people who are “antibody-positive” shows a huge variation within the five boroughs of the city. It is therefore possible that the harder hit areas, such as parts of Brooklyn and Queens, may be close to achieving a herd immunity threshold whereas other parts of the city may not (assuming that the antibody tests are accurate and antibodies are long-lasting). This is especially important to keep in mind because it clearly demonstrates that achieving a high percentage of immune individuals through natural infection is not an easy task and comes with a price (please refer to our past update on seropositivity from July 13, 2020).
We are interested in knowing what topics we should cover in future updates. Please share your thoughts with us by taking this short (1-2 minute) anonymous survey.
You can find information specific to your state or city or town on your health department’s website:
Directory of state department of health websites
Directory of local health department websites
American Medical Association resources for healthcare providers